Riesco-Martinez Maria Carmen, Capdevila Jaume, Alonso Vicente, Jimenez-Fonseca Paula, Teule Alex, Grande Enrique, Sevilla Isabel, Benavent Marta, Alonso-Gordoa Teresa, Custodio Ana, Anton-Pascual Beatriz, Hernando Jorge, Polo Eduardo, Castillo-Trujillo Oscar Alfredo, Lamas-Paz Arantza, Teijo Ana, Rodriguez-Gil Yolanda, Soldevilla Beatriz, Garcia-Carbonero Rocio
Medical Oncology Department. Hospital Universitario 12 de Octubre, Madrid, Spain.
Medical Oncology Department. Vall Hebron University Hospital, Vall Hebron Institute of Oncology (VHIO), Barcelona, Spain.
Nat Commun. 2024 Aug 8;15(1):6753. doi: 10.1038/s41467-024-50969-8.
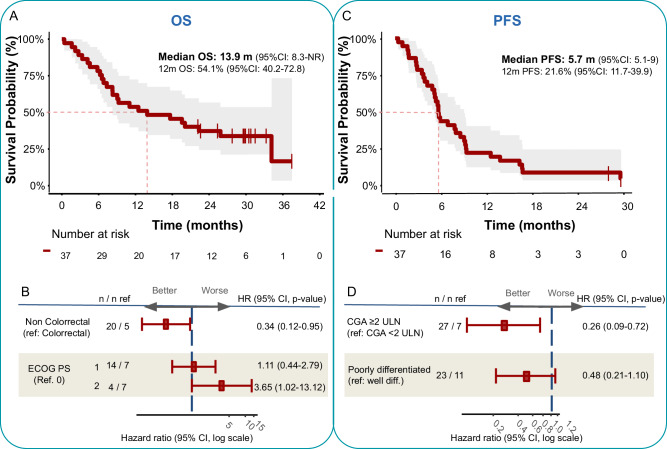
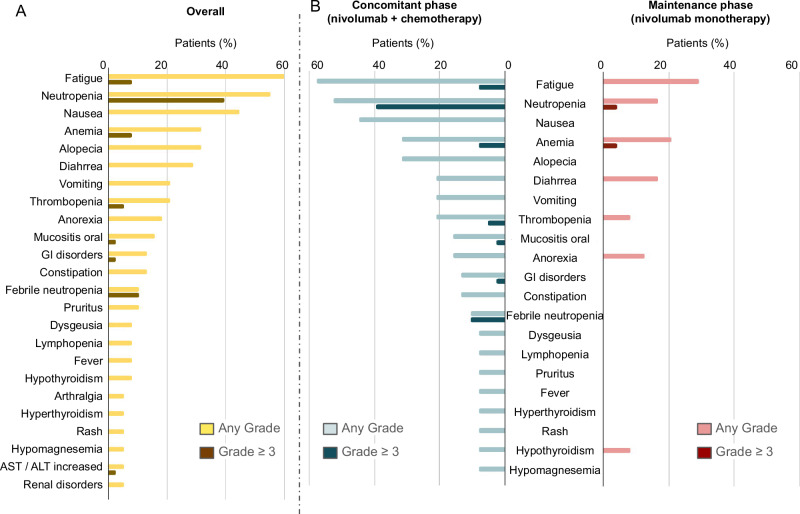
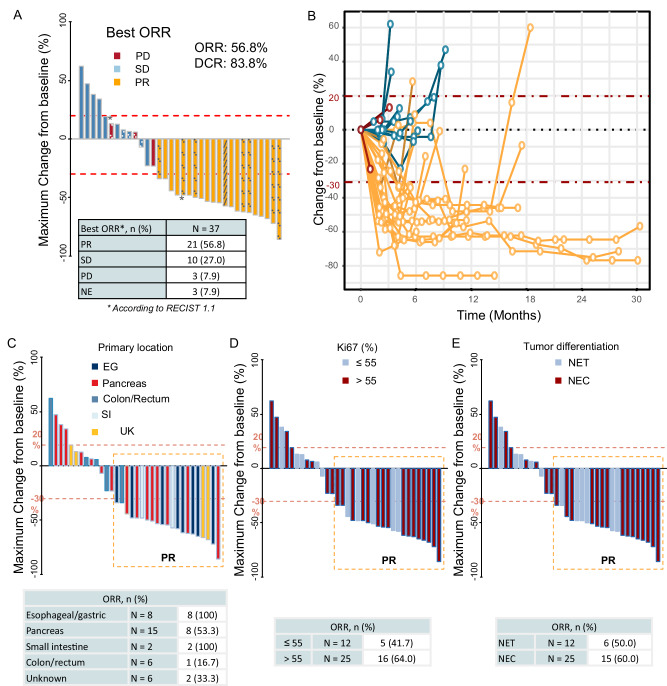
The prognosis of patients with advanced high-grade (G3) digestive neuroendocrine neoplasms (NENs) is rather poor. The addition of immune checkpoint inhibition to platinum-based chemotherapy may improve survival. NICE-NEC (NCT03980925) is a single-arm, phase II trial that recruited chemotherapy-naive, unresectable advanced or metastatic G3 NENs of gastroenteropancreatic (GEP) or unknown origin. Patients received nivolumab 360 mg intravenously (iv) on day 1, carboplatin AUC 5 iv on day 1, and etoposide 100 mg/m/d iv on days 1-3, every 3 weeks for up to six cycles, followed by nivolumab 480 mg every 4 weeks for up to 24 months, disease progression, death or unacceptable toxicity. The primary endpoint was the 12-month overall survival (OS) rate (H 50%, H 72%, β 80%, α 5%). Secondary endpoints were objective response rate (ORR), duration of response (DoR), progression-free survival (PFS), and safety. From 2019 to 2021, 37 patients were enrolled. The most common primary sites were the pancreas (37.8%), stomach (16.2%) and colon (10.8%). Twenty-five patients (67.6%) were poorly differentiated carcinomas (NECs) and/or had a Ki67 index >55%. The ORR was 56.8%. Median PFS was 5.7 months (95%CI: 5.1-9) and median OS 13.9 months (95%CI: 8.3-Not reached), with a 12-month OS rate of 54.1% (95%CI: 40.2-72.8) that did not meet the primary endpoint. However, 37.6% of patients were long-term survivors (>2 years). The safety profile was consistent with previous reports. There was one treatment-related death. Nivolumab plus platinum-based chemotherapy was associated with prolonged survival in over one-third of chemonaïve patients with G3 GEP-NENs, with a manageable safety profile.
晚期高级别(G3)消化神经内分泌肿瘤(NENs)患者的预后相当差。在铂类化疗基础上加用免疫检查点抑制剂可能会改善生存情况。NICE-NEC(NCT03980925)是一项单臂II期试验,招募了未经化疗、不可切除的晚期或转移性胃肠胰(GEP)或来源不明的G3 NENs患者。患者在第1天静脉注射(iv)纳武利尤单抗360mg,第1天静脉注射卡铂AUC 5,第1 - 3天静脉注射依托泊苷100mg/m²/天,每3周进行一次,共六个周期,之后每4周静脉注射纳武利尤单抗480mg,持续长达24个月,直至疾病进展、死亡或出现不可接受的毒性。主要终点是12个月总生存率(OS)(H = 50%,H = 72%,β = 80%,α = 5%)。次要终点是客观缓解率(ORR)、缓解持续时间(DoR)、无进展生存期(PFS)和安全性。2019年至2021年,共纳入37例患者。最常见的原发部位是胰腺(37.8%)、胃(16.2%)和结肠(10.8%)。25例患者(67.6%)为低分化癌(NECs)和/或Ki67指数>55%。ORR为56.8%。中位PFS为5.7个月(95%CI:5.1 - 9),中位OS为13.9个月(95%CI:8.3 - 未达到),12个月OS率为54.1%(95%CI:40.2 - 72.8),未达到主要终点。然而,37.6%的患者为长期生存者(>2年)。安全性与既往报道一致。有1例与治疗相关的死亡。纳武利尤单抗联合铂类化疗使超过三分之一的初治G3 GEP - NENs患者生存期延长,且安全性可控。