Dykes Kaitlyn C, Chou Jiling, Taylor Allison O, Shu Albert C, Mudra Sarah E, Ma Xiaoyang, Ahn Jaeil, Lai Catherine E
Department of Medicine, MedStar Georgetown University Hospital, Washington, DC, USA.
Department of Medicine, Division of Hematology and Oncology, University of California San Diego Moores Cancer Center, San Diego, California, USA.
Cancer Rep (Hoboken). 2024 Aug;7(8):e2162. doi: 10.1002/cnr2.2162.
It is important to understand the outcomes of adult acute lymphoblastic leukemia (ALL) patients at different facilities as treatment paradigms change.
Our primary objective was to determine adult ALL overall survival (OS) by facility volume and type. Secondary objectives included identifying sociodemographic factors that may have impacted outcomes and analyzing treatment patterns by facility volume and type.
This was a retrospective analysis of the National Cancer Database (NCDB) that included patients ≥40 years diagnosed with ALL between 2004 and 2016.
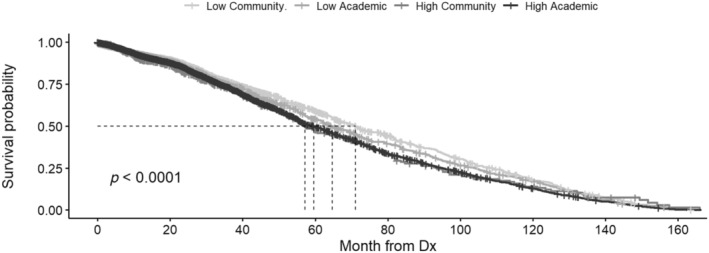
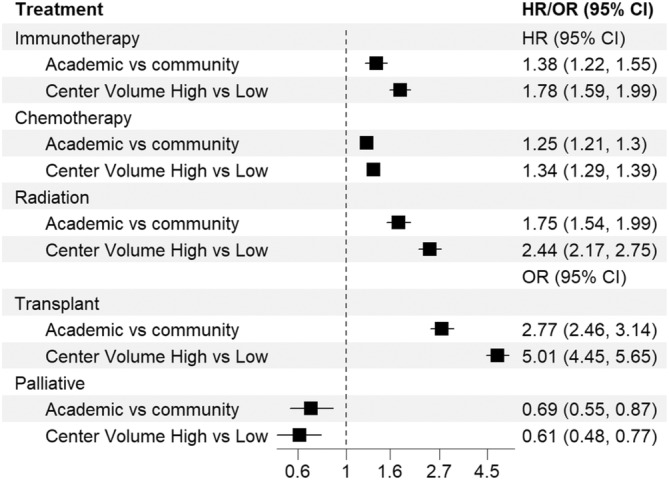
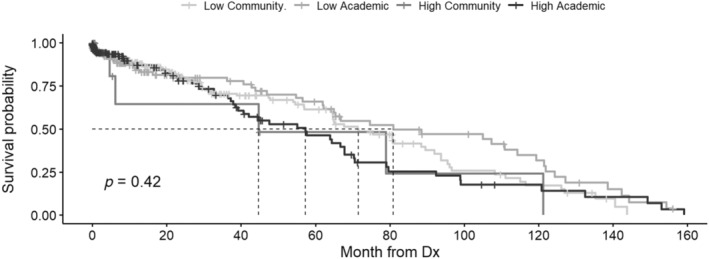
A total of 14 593 patients were included in this study. Univariate OS was greatest at low volume (LV) and community programs (CPs) and the least at high volume (HV) and academic programs (AP). This difference was lost after multivariable Cox proportional hazards model analysis, which found no difference in survival by facility volume or type, however, survival was significantly influenced by age, race, Hispanic ethnicity, insurance, and residence location (p < 0.05). Patients treated at HV and APs compared to LV and CP received more anti-neoplastic directed therapy.
Our results suggest treatment facility volume and type do not impact older adult ALL patient (≥40 years) survival, however confounding sociodemographic differences do impact survival outcomes, despite more aggressive and novel treatment approaches provided at HV and APs.
随着治疗模式的改变,了解不同医疗机构中成人急性淋巴细胞白血病(ALL)患者的治疗结果很重要。
我们的主要目标是按医疗机构规模和类型确定成人ALL的总生存期(OS)。次要目标包括确定可能影响治疗结果的社会人口统计学因素,并按医疗机构规模和类型分析治疗模式。
这是一项对国家癌症数据库(NCDB)的回顾性分析,纳入了2004年至2016年间诊断为ALL的40岁及以上患者。
本研究共纳入14593例患者。单因素分析显示,低容量(LV)和社区项目(CP)的总生存期最长,高容量(HV)和学术项目(AP)的总生存期最短。多变量Cox比例风险模型分析后这种差异消失,该分析发现按医疗机构规模或类型生存无差异,然而,生存受到年龄、种族、西班牙裔、保险和居住地点的显著影响(p<0.05)。与LV和CP相比,在HV和AP接受治疗的患者接受了更多的抗肿瘤定向治疗。
我们的结果表明,治疗机构的规模和类型不会影响老年成人ALL患者(≥40岁)的生存,然而,尽管HV和AP提供了更积极和新颖的治疗方法,但混杂的社会人口统计学差异确实会影响生存结果。