van Gennep Erik J, Claps Francesco, Bostrom Peter J, Shariat Shahrokh F, Neuzillet Yann, Zlotta Alexandre R, Trombetta Carlo, Eckstein Markus, Mertens Laura S, Bussani Rossana, Burger Maximilian, Boormans Joost L, Wullich Bernd, Hartmann Arndt, Mayr Roman, Pavan Nicola, Bartoletti Riccardo, Mir M Carmen, Pouessel Damien, van der Hoeven John, van der Kwast Theo H, Allory Yves, Zuiverloon Tahlita C M, Lotan Yair, van Rhijn Bas W G
Department of Surgical Oncology (Urology), Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands.
Department of Urology, Leiden University Medical Center, Leiden, The Netherlands.
Bladder Cancer. 2024 Jun 18;10(2):119-132. doi: 10.3233/BLC-230086. eCollection 2024.
Prognostic tools in pathological-node (pN) patients after radical cystectomy (RC) are needed.
To evaluate the prognostic impact of lymph node (LN)-density on disease-specific survival (DSS) in patients with bladder cancer (BC) undergoing RC with pelvic lymph node dissection.
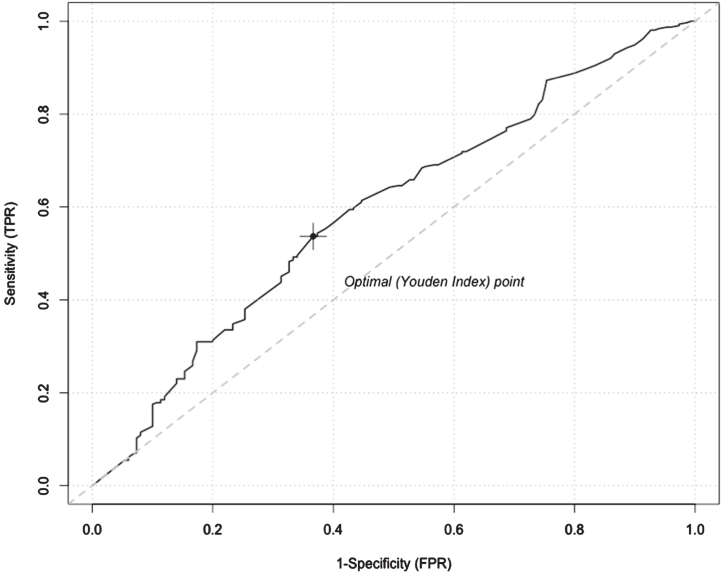
We analyzed a multi-institutional cohort of 1169 patients treated with upfront RC for cT1-4aN0M0 urothelial BCat nine centers. LN-densitywas calculated as the ratio of the number of positive LNs×100% to the number of LNs removed. The optimal LN-density cut-off value was defined by creating a time-dependent receiver operating characteristic (ROC) curve in pN patients. Univariable and multivariable Cox' regression analyses were used to assess the effect of conventional Tumor Nodes Metastasis (TNM) nodal staging system, LN-density and other LN-related variables on DSS in the pN-positive cohort.
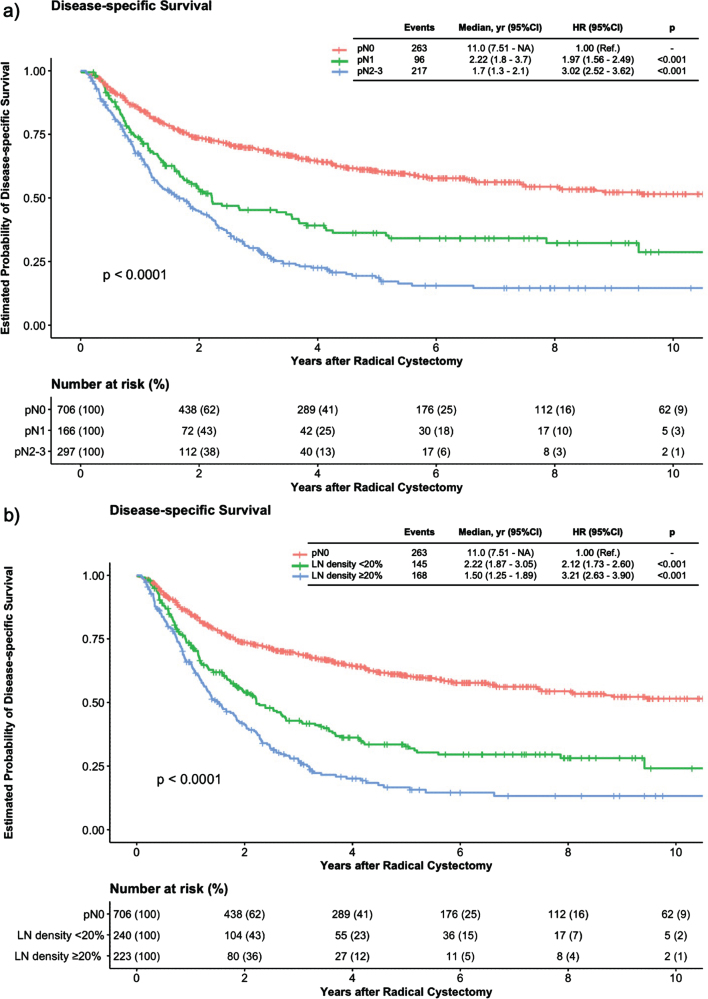
Of the 1169 patients, 463 (39.6%) patients had LN-involvement. The area under the ROC curve was 0.60 and the cut-off for LN-density was set at 20%, 223 of the pN-positive patients (48.2%) had a LN-density ≥ 20%. In multivariable models, the number of LN-metastases (HR 1.03, p = 0.005) and LN-density, either as continuous (HR 1.01, p = 0.013) or as categorical variable (HR 1.37, p = 0.014), were independently associated with worse DSS, whereas pN-stage was not.
LN-density ≥ 20% was an independent predictor of worse DSS in BC patients with LN-involvement at RC. The integration of LN-density and other LN-parameters rather than only conventional pN-stage may contribute to a more refined risk-stratification in BC patients with nodal involvement.
根治性膀胱切除术(RC)后病理分期为淋巴结阳性(pN)的患者需要预后评估工具。
评估淋巴结(LN)密度对接受盆腔淋巴结清扫的膀胱癌(BC)患者行RC后的疾病特异性生存(DSS)的预后影响。
我们分析了来自九个中心的1169例接受 upfront RC 治疗的 cT1-4aN0M0 尿路上皮 BC 患者的多机构队列。LN 密度计算为阳性 LN 数量×100%与切除的 LN 数量的比值。通过在 pN 患者中创建时间依赖性受试者操作特征(ROC)曲线来定义最佳 LN 密度临界值。采用单变量和多变量 Cox 回归分析评估传统肿瘤淋巴结转移(TNM)淋巴结分期系统、LN 密度和其他 LN 相关变量对 pN 阳性队列中 DSS 的影响。
1169例患者中,463例(39.6%)有LN转移。ROC曲线下面积为0.60,LN密度临界值设定为20%,223例pN阳性患者(48.2%)的LN密度≥20%。在多变量模型中,LN转移数量(HR 1.03,p = 0.005)和LN密度,无论是作为连续变量(HR 1.01,p = 0.013)还是分类变量(HR 1.37,p = 0.014),均与较差的DSS独立相关,而pN分期则不然。
LN密度≥20%是RC时伴有LN转移的BC患者DSS较差的独立预测因素。整合LN密度和其他LN参数而非仅传统的pN分期可能有助于对有淋巴结受累的BC患者进行更精确的风险分层。