Ahmad Yousif, Oakley Luke, Yoon Sunghan, Kaewkes Danon, Chakravarty Tarun, Patel Chinar, Palmerini Tullio, Bruno Antonio G, Saia Francesco, Testa Luca, Bedogni Francesco, Chieffo Alaide, Montorfano Matteo, Bartorelli Antonio L, Porto Italo, Grube Eberhard, Nickenig Georg, Sinning Jan-Malte, De Carlo Marco, Petronio Anna Sonia, Barbanti Marco, Tamburino Corrado, Iadanza Alessandro, Burzotta Francesco, Trani Carlo, Fraccaro Chiara, Tarantini Giuseppe, Aranzulla Tiziana C, Musumeci Giuseppe, Stefanini Giulio G, Taramasso Maurizio, Kim Hyo-Soo, Codner Pablo, Kornowski Ran, Pelliccia Francesco, Vignali Luigi, Makkar Raj R
Yale School of Medicine, Yale University, New Haven, Connecticut.
Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, California.
J Soc Cardiovasc Angiogr Interv. 2022 Jun 22;1(4):100347. doi: 10.1016/j.jscai.2022.100347. eCollection 2022 Jul-Aug.
Coronary obstruction following transcatheter aortic valve replacement (TAVR) is a life-threatening complication. For patients at elevated risk, it is not known how valve choice is influenced by clinical and anatomic factors and how outcomes differ between valve platforms. For patients at high risk of coronary obstruction, we sought to describe the anatomical and clinical characteristics of patients treated with both balloon-expandable (BE) and self-expanding (SE) valves.
This was a multicenter international registry of patients undergoing TAVR who are considered to be at high risk of coronary obstruction and receiving pre-emptive coronary protection.
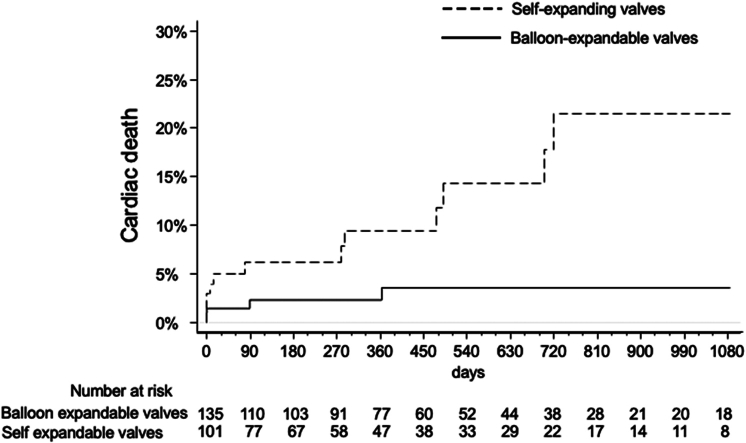
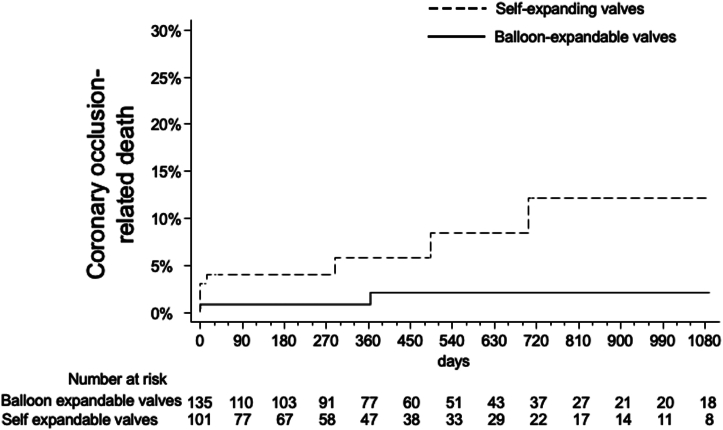
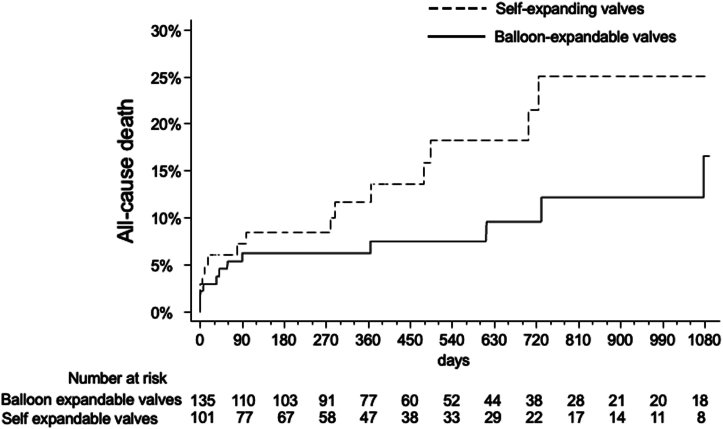
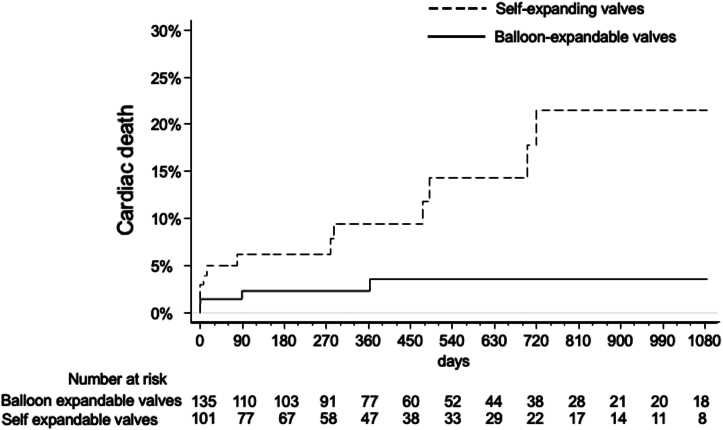
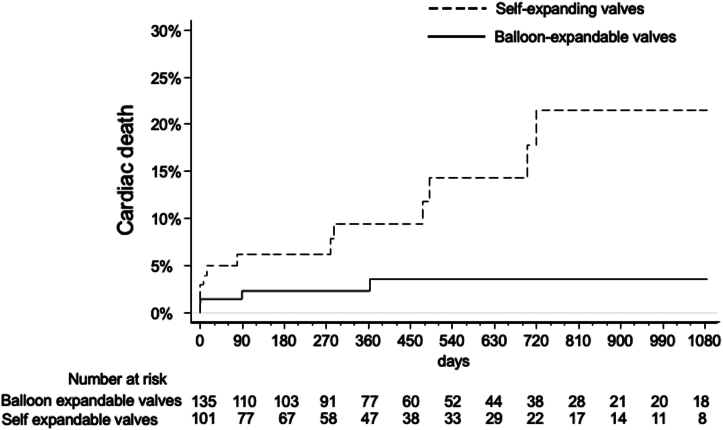
A total of 236 patients were included. Patients receiving SE valves were more likely to undergo valve-in-valve procedures and also had smaller sinuses of Valsalva and valve-to-coronary distance. Three-year cardiac mortality was 21.6% with SE vs 3.7% with BE valves. This was primarily driven by increased rates of definite or probable coronary occlusion, which occurred in 12.1% of patients with SE valves vs 2.1% in patients with BE valves.
In patients undergoing TAVR with coronary protection, those treated with SE valves had increased rates of clinical and anatomic features that increase the risk of coronary obstruction. These include an increased frequency of valve-in-valve procedures, smaller sinuses of Valsalva, and smaller valve-to-coronary distances. These patients were observed to have increased cardiac mortality compared with patients treated with BE valves, but this is likely due to their higher risk clinical and anatomic phenotypes rather than as a function of the valve type itself.
经导管主动脉瓣置换术(TAVR)后冠状动脉阻塞是一种危及生命的并发症。对于高危患者,尚不清楚临床和解剖因素如何影响瓣膜选择,以及不同瓣膜平台的结局有何差异。对于冠状动脉阻塞高危患者,我们试图描述接受球囊扩张式(BE)瓣膜和自膨胀式(SE)瓣膜治疗患者的解剖和临床特征。
这是一项多中心国际注册研究,纳入了被认为有冠状动脉阻塞高危且接受预防性冠状动脉保护的TAVR患者。
共纳入236例患者。接受SE瓣膜的患者更有可能接受瓣中瓣手术,并且其主动脉瓣窦较小,瓣膜至冠状动脉距离较短。SE瓣膜组的三年心脏死亡率为21.6%,而BE瓣膜组为3.7%。这主要是由于明确或可能的冠状动脉闭塞发生率增加所致,SE瓣膜组患者中发生率为12.1%,而BE瓣膜组患者中为2.1%。
在接受冠状动脉保护的TAVR患者中,接受SE瓣膜治疗的患者出现增加冠状动脉阻塞风险的临床和解剖特征的发生率更高。这些特征包括瓣中瓣手术频率增加、主动脉瓣窦较小以及瓣膜至冠状动脉距离较短。与接受BE瓣膜治疗的患者相比,观察到这些患者的心脏死亡率增加,但这可能是由于其更高风险的临床和解剖表型,而非瓣膜类型本身的作用。