Gidwani Risha, Yank Veronica, Burgette Lane, Kofner Aaron, Asch Steven M, Wagner Zachary
Economics, Sociology, and Statistics (ESS), RAND Corporation, Santa Monica, California, USA.
Fielding School of Public Health, University of California Los Angeles (UCLA), Los Angeles, California, USA.
Health Serv Res. 2024 Dec;59(6):e14343. doi: 10.1111/1475-6773.14343. Epub 2024 Aug 13.
Evaluate whether cost-sharing decreases led high-deductible health plans (HDHP) enrollees to increase their use of healthcare.
DATA SOURCES, STUDY SETTING: National sample of chronically-ill patients age 18-64 from 2018 to 2020 (n = 1,318,178).
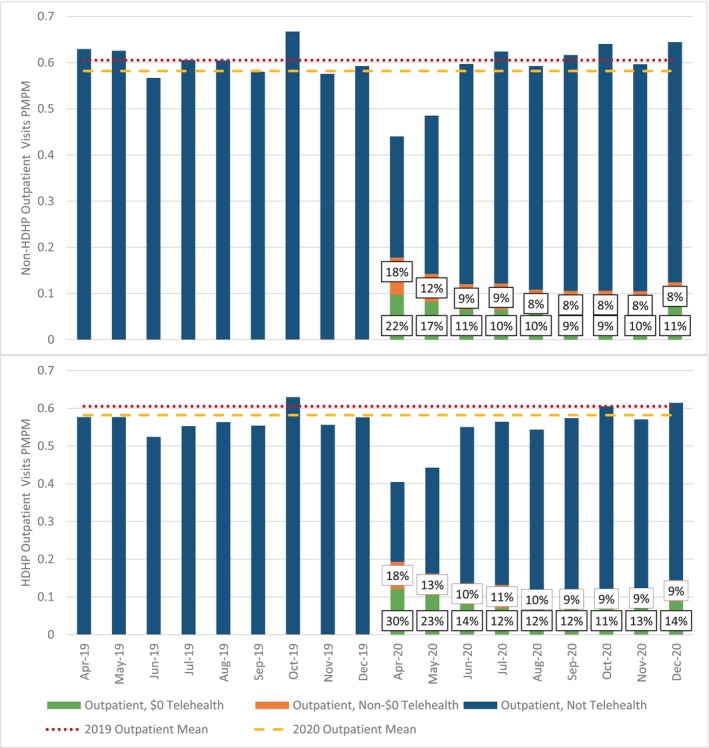
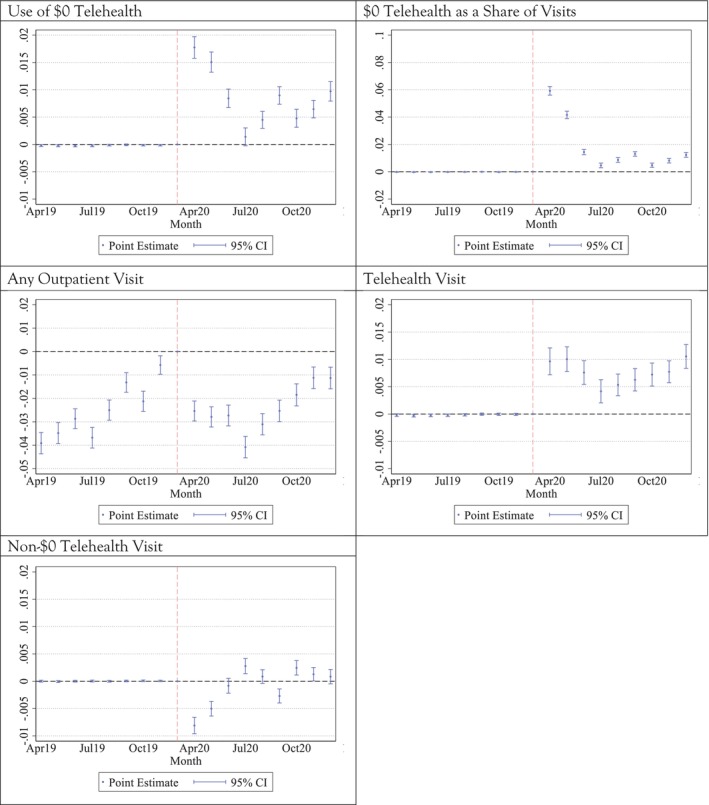
Difference-in-differences analyses using entropy-balancing weights were used to evaluate the effect of a policy shift to $0 cost-sharing for telehealth on utilization for HDHP compared with non-HDHP enrollees. Due to this shock, HDHP enrollees experienced substantial declines in cost-sharing for telehealth, while non-HDHP enrollees experienced small declines. Event study models were also used to evaluate changes over time.
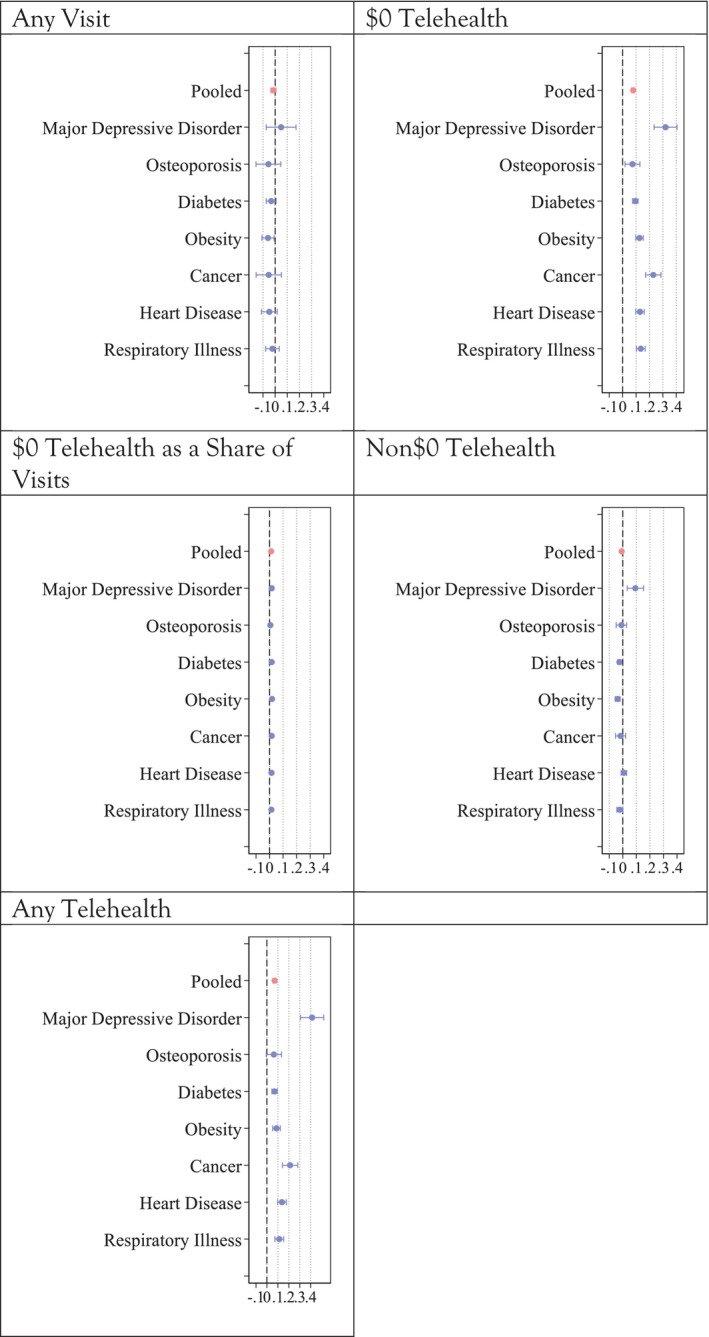
DATA COLLECTION/EXTRACTION METHODS: Outcomes included use of any outpatient care; use of $0 telehealth; use of $0 telehealth as a proportion of all outpatient care; and use of any telehealth. To test whether any differences were due to preferences for care modality versus cost-sharing, we further evaluated use of non-$0 telehealth as a placebo test.
There was no difference in change in overall outpatient visits (p = 0.84), with chronicall-ill HDHP enrollees using less care both before and after the policy shift. However, compared with non-HDHP enrollees, HDHP enrollees increased their use of $0 telehealth by 0.08 visits over a 9-month period, a 27% increase (95% CI 0.07-0.09, p < 0.001) and shifted 1.2 percentage points more of their care to $0 telehealth, a 15% increase (ß = 0.01, 95% CI 0.01, 0.01, p < 0.001). However, HDHP enrollees had lower uptake of non-$0 telehealth than non-HDHP enrollees (ß = -0.01, 95%CI -0.02, 0.00, p = 0.04).
Recent-but-expiring federal legislation exempts telehealth from HDHP deductibles for care provided in 2023 and 2024. Our results indicate that extending the protections provided by this legislation could help reduce the gap in access to care for chronically-ill persons enrolled in HDHPs.
评估费用分摊的降低是否会导致高免赔额健康保险计划(HDHP)的参保者增加医疗保健的使用。
数据来源、研究背景:2018年至2020年18 - 64岁慢性病患者的全国样本(n = 1,318,178)。
使用熵平衡权重的差异分析来评估远程医疗零费用分摊政策转变对HDHP参保者与非HDHP参保者医疗利用率的影响。由于这一冲击,HDHP参保者的远程医疗费用分摊大幅下降,而非HDHP参保者的费用分摊下降幅度较小。还使用事件研究模型来评估随时间的变化。
数据收集/提取方法:结果包括任何门诊护理的使用;零费用远程医疗的使用;零费用远程医疗占所有门诊护理的比例;以及任何远程医疗的使用。为了测试任何差异是否是由于对护理方式的偏好而非费用分摊,我们进一步评估了非零费用远程医疗的使用作为安慰剂测试。
总体门诊就诊次数的变化没有差异(p = 0.84),慢性病HDHP参保者在政策转变前后的护理使用都较少。然而,与非HDHP参保者相比,HDHP参保者在9个月内零费用远程医疗的使用增加了0.08次就诊,增加了27%(95%置信区间0.07 - 0.09,p < 0.001),并且将其护理的1.2个百分点更多地转向零费用远程医疗,增加了15%(β = 0.01,95%置信区间0.01,0.01,p < 0.001)。然而,HDHP参保者对非零费用远程医疗的接受程度低于非HDHP参保者(β = -0.01,95%置信区间 -0.02,0.00,p = 0.04)。
近期但即将到期的联邦立法豁免了2023年和2024年提供的远程医疗在HDHP免赔额方面的费用。我们的结果表明,延长该立法提供的保护措施有助于缩小参加HDHP的慢性病患者在获得护理方面的差距。