Oncologic Dermatology Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Department of Medical and Surgical Sciences (DIMEC), Alma Mater Studiorum University of Bologna, Bologna, Italy.
Skin Res Technol. 2024 Aug;30(8):e70012. doi: 10.1111/srt.70012.
Basosquamous carcinoma (BSC) is a rare and aggressive nonmelanoma skin cancer (NMSC) that exhibits features of both BCC and squamous cell carcinoma (SCC). The gold standard for diagnosis is histopathological examination. BSC is often challenging to diagnose and manage due to its mixed histological features and potential for aggressive behavior AIM: To identify specific features aiding clinicians in differentiating BSCs using non-invasive diagnostic techniques.
We conducted a retrospective descriptive, monocentric study of the epidemiological clinical, dermoscopic, and reflectance confocal microscopy (RCM) features of histopathologically proven BSCs diagnosed between 2010 and 2023. A total of 192 cases were selected.
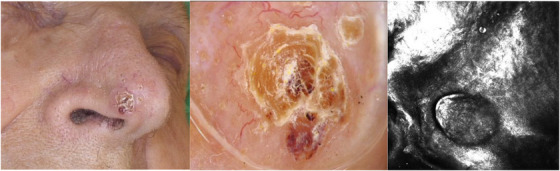
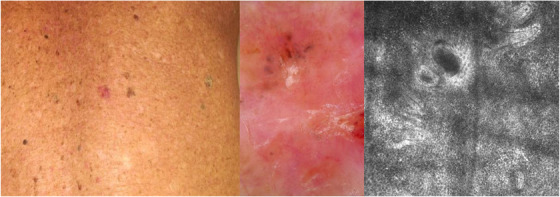
The study population consisted of 17 men (60.9%). Total 95.8% of patients at the time of diagnosis were ≥50 years. BSC occurred in the head and neck area in 124 cases (63.1%) of which 65 (33.9%) were in the H-zone. For 47.4% of patients, BSC presented as a macule with undefined clinical margins (43.3%). Dermoscopic images were available for 98 cases: the most common parameter was the presence of whitish structureless areas (59 [60.2%]), keratin masses (58 [59.2%]), superficial scales, and ulceration or blood crusts (49 [50%] both). Vessels pattern analysis revealed hairpin vessels (exclusively) and linear irregular vessels as the most frequent (55 [56.1%] both). RCM examination was performed in 21 cases which revealed specific SCC features such as solar elastosis (19 [90.5%]), atypical honeycomb pattern (17 [89%]), proliferation of atypical keratinocytes (16 [80%]) combined with BCC' ones as bright tumor islands (12 [57.8%]), and cleft-like dark spaces (11 [53.4%]).
Our study reflects the largest cohort of BSCs from a single institution. We described an incidence rate of 4.7%, higher than reported in the Literature, with the involvement of patients ≥50years in almost 96% of cases and an overall male predominance. At clinical examination, BSC was described as a hyperkeratotic macule with undefined clinical margins with one or more dermoscopic SCC' features, whereas the presence of typical BCC aspects was observed in less than 10% of cases, differently from what was previously reported. At RCM analysis, BSCs presented with an atypical honeycomb pattern with proliferation of atypical keratinocytes, hyperkeratosis, and in nearly 55% of patients, bright tumor islands with cleft-like dark spaces.
The distinctive dermoscopic patterns, along with the RCM features aid in the differentiation of BSCs from other NMSCs.
基底鳞状细胞癌(BSC)是一种罕见且侵袭性的非黑色素瘤皮肤癌(NMSC),具有基底细胞癌(BCC)和鳞状细胞癌(SCC)的特征。诊断的金标准是组织病理学检查。由于其混合的组织学特征和潜在的侵袭性行为,BSC 的诊断和管理具有挑战性。
确定有助于临床医生使用非侵入性诊断技术区分 BSCs 的特定特征。
我们对 2010 年至 2023 年间病理证实的 BSC 进行了回顾性描述性、单中心研究,包括流行病学、临床、皮肤镜和反射共聚焦显微镜(RCM)特征。共选择了 192 例病例。
研究人群包括 17 名男性(60.9%)。95.8%的患者在诊断时年龄≥50 岁。BSC 发生在头部和颈部区域 124 例(63.1%),其中 H 区 65 例(33.9%)。47.4%的患者表现为边界不明确的斑疹(43.3%)。98 例患者有皮肤镜图像:最常见的参数是存在白色无结构区域(59 [60.2%])、角蛋白块(58 [59.2%])、浅表鳞屑和溃疡或血痂(49 [50%])。血管模式分析显示发夹状血管(单独)和线性不规则血管是最常见的(55 [56.1%])。对 21 例患者进行了 RCM 检查,发现了特定的 SCC 特征,如太阳弹性纤维变性(19 [90.5%])、非典型蜂窝状模式(17 [89%])、非典型角朊细胞增生(16 [80%])与 BCC 的明亮肿瘤岛(12 [57.8%])和裂隙状暗区(11 [53.4%])相结合。
我们的研究反映了来自单一机构的最大 BSC 队列。我们描述了发病率为 4.7%,高于文献报道,几乎 96%的病例涉及≥50 岁的患者,总体上男性占优势。在临床检查中,BSC 被描述为边界不明确的角化过度斑疹,具有一个或多个皮肤镜 SCC 特征,而在不到 10%的病例中观察到典型的 BCC 特征,这与之前的报道不同。在 RCM 分析中,BSC 表现为非典型蜂窝状模式,伴有非典型角朊细胞增生、角化过度,近 55%的患者出现有裂隙状暗区的明亮肿瘤岛。
独特的皮肤镜模式以及 RCM 特征有助于将 BSCs 与其他 NMSC 区分开来。