Chatani Ryuki, Kubo Shunsuke, Tasaka Hiroshi, Sakata Atsushi, Yoshino Mitsuru, Maruo Takeshi, Kadota Kazushige
Department of Cardiovascular Medicine Kurashiki Central Hospital Kurashiki Japan.
J Arrhythm. 2024 May 23;40(4):879-890. doi: 10.1002/joa3.13073. eCollection 2024 Aug.
Patients with atrial fibrillation (AF) who are not suitable for long-term anticoagulant therapy undergo percutaneous left atrial appendage closure (LAAC). The safety and feasibility of left atrial catheter ablation (CA) procedures after LAAC remain unclear. This study aimed to clarify the feasibility and safety of CA after LAAC, including in the early phase within 180 days.
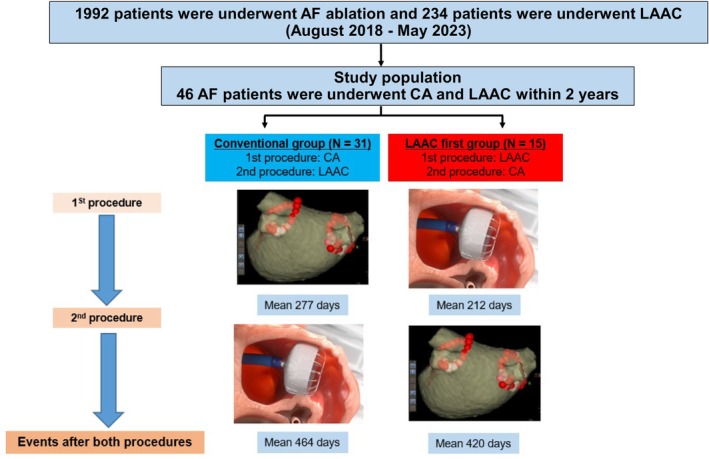
Characteristics and clinical outcomes of 46 patients with AF who had undergone both CA and LAAC within 2 years (mean age, 72 years; 29 men) were compared between those who had undergone CA-first (31 patients) and LAAC-first (15 patients).
The mean CHA₂DS₂-VASc and HAS-BLED scores were 4.8 and 3.3 points, respectively. The LAAC-first strategy was often used in patients with prior major bleeding and LAA thrombosis or sludge. In the LAAC-first group, the mean duration between both procedures was 212 days, and all LAAC-first patients, including seven patients in the early phase, could undergo CA without LAAC device-related complications; moreover, no cardiovascular adverse events were reported after both procedures (mean periods: 420 days). After CA post-LAAC, no device-related adverse events (device-related thrombosis, new peri-device leak appearance, peri-device leak increase, or device dislodgement) were observed, whereas, after LAAC post-CA, 3 new peri-device leak appearance events and 1 peri-device leak increase event were observed, especially patients who underwent LAAC in the early phase post-CA.
Based on single-center experience, left atrial CA in the presence of an LAAC device implanted including the early phase was safe and feasible.
不适合长期抗凝治疗的心房颤动(AF)患者接受经皮左心耳封堵术(LAAC)。LAAC术后左心房导管消融(CA)手术的安全性和可行性仍不明确。本研究旨在阐明LAAC术后CA的可行性和安全性,包括180天内的早期阶段。
比较46例在2年内同时接受CA和LAAC的AF患者(平均年龄72岁;29例男性)的特征和临床结局,这些患者分为先进行CA组(31例患者)和先进行LAAC组(15例患者)。
平均CHA₂DS₂-VASc和HAS-BLED评分分别为4.8分和3.3分。先进行LAAC策略常用于既往有大出血、左心耳血栓形成或淤滞的患者。在先进行LAAC组中,两次手术之间的平均间隔时间为212天,所有先进行LAAC的患者,包括7例早期患者,均可在无LAAC装置相关并发症的情况下接受CA;此外,两次手术后均未报告心血管不良事件(平均随访期:420天)。LAAC术后CA后,未观察到与装置相关的不良事件(装置相关血栓形成、新的装置周围漏血出现、装置周围漏血增加或装置移位),而CA术后LAAC后,观察到3例新的装置周围漏血出现事件和1例装置周围漏血增加事件,尤其是在CA术后早期接受LAAC的患者。
基于单中心经验,在植入LAAC装置的情况下,包括早期阶段在内的左心房CA是安全可行的。