Department of Anesthesiology, Intensive Care and Pain Medicine, BG Klinikum Unfallkrankenhaus Berlin, Warener Strasse 7, 12683, Berlin, Germany.
Department of Trauma and Orthopaedic Surgery, BG Klinikum Unfallkrankenhaus Berlin, Warener Strasse 7, 12683, Berlin, Germany.
Scand J Trauma Resusc Emerg Med. 2024 Aug 14;32(1):70. doi: 10.1186/s13049-024-01239-5.
Prehospital management of severely burned patients is extremely challenging. It should include adequate analgesia, decision-making on the necessity of prehospital endotracheal intubation and the administration of crystalloid fluids. Guidelines recommend immediate transport to specialised burn centres when certain criteria are met. To date, there is still insufficient knowledge on the characteristics of prehospital emergency treatment. We sought to investigate the current practice and its potential effects on patient outcome.
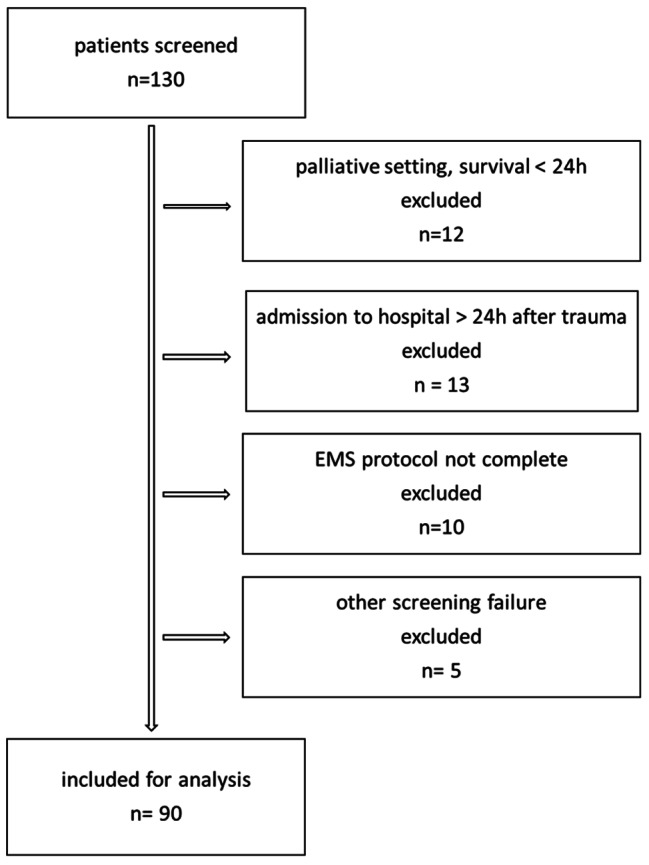
We conducted a single centre, retrospective cohort analysis of severely burned patients (total burned surface area > 20%), admitted to the Berlin burn centre between 2014 and 2019. The relevant data was extracted from Emergency Medical Service reports and digital patient charts for exploratory data analysis. Primary outcome was 28-day-mortality.
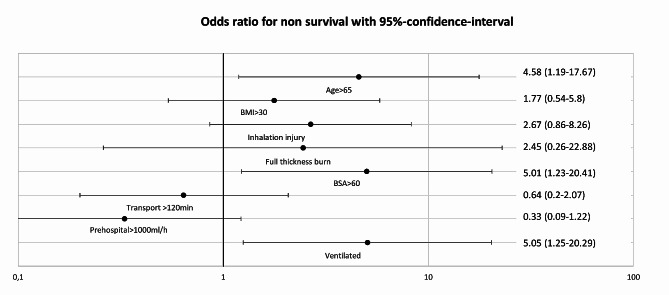
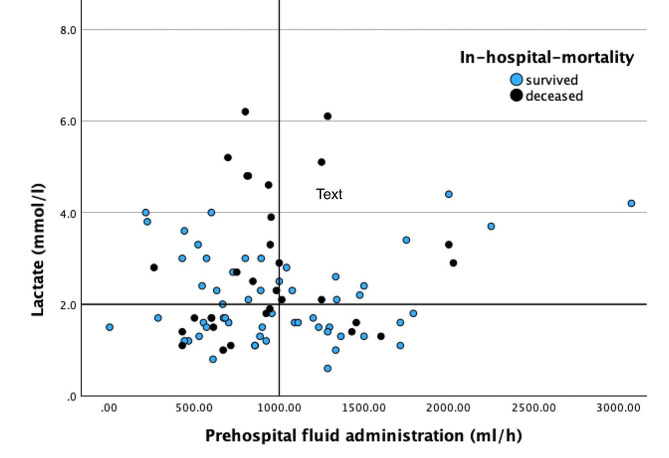
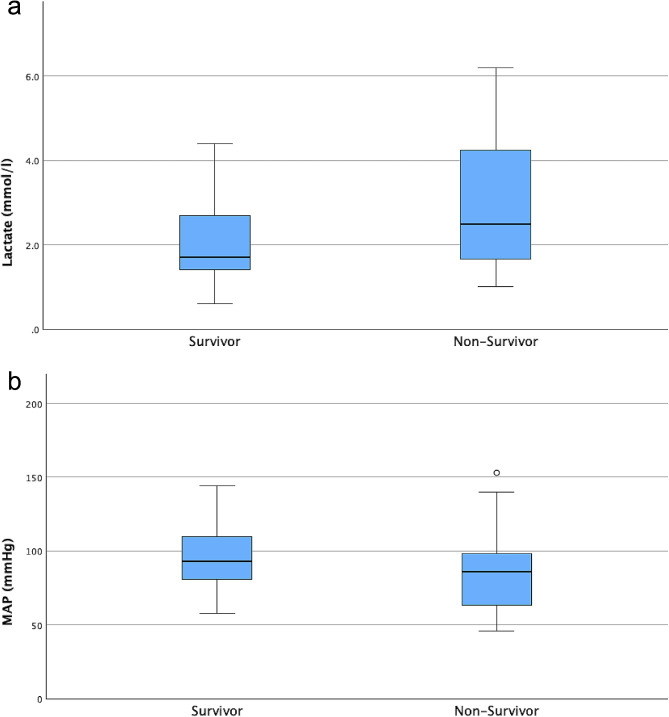
Ninety patients (male/female 60/30, with a median age of 52 years [interquartile range, IQR 37-63], median total burned surface area 36% [IQR 25-51] and median body mass index 26.56 kg/m [IQR 22.86-30.86] were included. The median time from trauma to ED arrival was 1 h 45 min; within this time, on average 1961 ml of crystalloid fluid (0.48 ml/kg/%TBSA, IQR 0.32-0.86) was administered. Most patients received opioid-based analgesia. Times from trauma to ED arrival were longer for patients who were intubated. Neither excessive fluid treatment (> 1000 ml/h) nor transport times > 2 h was associated with higher mortality. A total of 31 patients (34,4%) died within the hospital stay. Multivariate regression analysis revealed that non-survival was linked to age > 65 years (odds ratio (OR) 3.5, 95% CI: 1.27-9.66), inhalation injury (OR 3.57, 95% CI: 1.36-9.36), burned surface area > 60% (OR 5.14, 95% CI 1.57-16.84) and prehospital intubation (5.38, 95% CI: 1.92-15.92).
We showed that severely burned patients frequently received excessive fluid administration prehospitally and that this was not associated with more hemodynamic stability or outcome. In our cohort, patients were frequently intubated prehospitally, which was associated with increased mortality rates. Further research and emergency medical staff training should focus on adequate fluid application and cautious decision-making on the risks and benefits of prehospital intubation.
German Clinical Trial Registry (ID: DRKS00033516).
严重烧伤患者的院前管理极具挑战性。这应包括充分的镇痛、决定是否需要院前气管插管以及给予晶体液。指南建议,当满足某些标准时,应立即将患者转运至专门的烧伤中心。迄今为止,对于院前急救的特点,我们的了解仍然不足。我们旨在研究目前的实践及其对患者预后的潜在影响。
我们对 2014 年至 2019 年期间在柏林烧伤中心收治的总烧伤面积>20%的严重烧伤患者进行了单中心回顾性队列分析。从紧急医疗服务报告和数字患者病历中提取相关数据,进行探索性数据分析。主要结局为 28 天死亡率。
共纳入 90 例患者(男/女 60/30 例,中位年龄 52 岁[四分位距(IQR)37-63],中位总烧伤面积 36%[IQR 25-51],中位体重指数 26.56kg/m[IQR 22.86-30.86])。从创伤到急诊科到达的中位时间为 1 小时 45 分钟;在此期间,平均给予 1961ml 晶体液(0.48ml/kg/%TBSA,IQR 0.32-0.86)。大多数患者接受了基于阿片类药物的镇痛。需要插管的患者从创伤到急诊科到达的时间更长。液体治疗过多(>1000ml/h)或转运时间>2 小时均与死亡率升高无关。共有 31 例患者(34.4%)在住院期间死亡。多变量回归分析显示,非生存与年龄>65 岁(比值比(OR)3.5,95%置信区间(CI):1.27-9.66)、吸入性损伤(OR 3.57,95%CI:1.36-9.36)、烧伤面积>60%(OR 5.14,95%CI 1.57-16.84)和院前插管(OR 5.38,95%CI:1.92-15.92)相关。
我们表明,严重烧伤患者经常在院前接受过多的液体治疗,这与更稳定的血流动力学或结局无关。在我们的队列中,患者经常在院前接受插管,这与死亡率升高有关。进一步的研究和急救医护人员培训应侧重于适当的液体应用,并谨慎决策院前插管的风险和益处。
德国临床试验注册处(ID:DRKS00033516)。