Zhong Lishan, Huang Yanyin, Xiao Shuo, Wang Zhenzhong, Li Yuxin, Zhao Junfei, Fang Dou, Wang Qiuji, Zhang Zhaolong, Huang Huanlei
Guangdong Cardiovascular Institute, Guangdong Provincial People's Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, China.
Guangdong Cardiovascular Institute, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China.
Quant Imaging Med Surg. 2024 Aug 1;14(8):5946-5960. doi: 10.21037/qims-23-1768. Epub 2024 Jul 30.
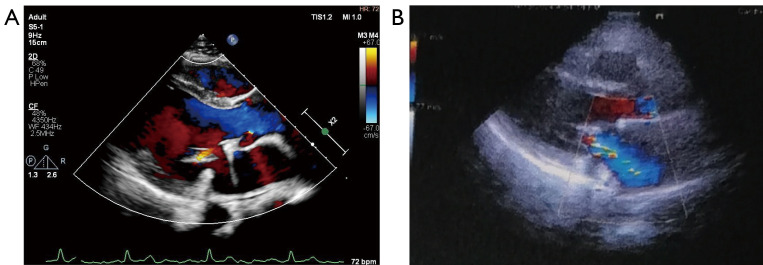
Barlow's disease (BD) is a common etiology of degenerative mitral valve (MV) disease, often causing significant mitral regurgitation (MR). The pathology of BD is challenging for surgeons performing MV repair (MVR). However, most MVR effectiveness studies have been based on survival and risk of reoperation. The aim of this study was to analyze the safety, efficacy, and durability of MVR in patients with BD and to identify factors that influence recurrent MR.
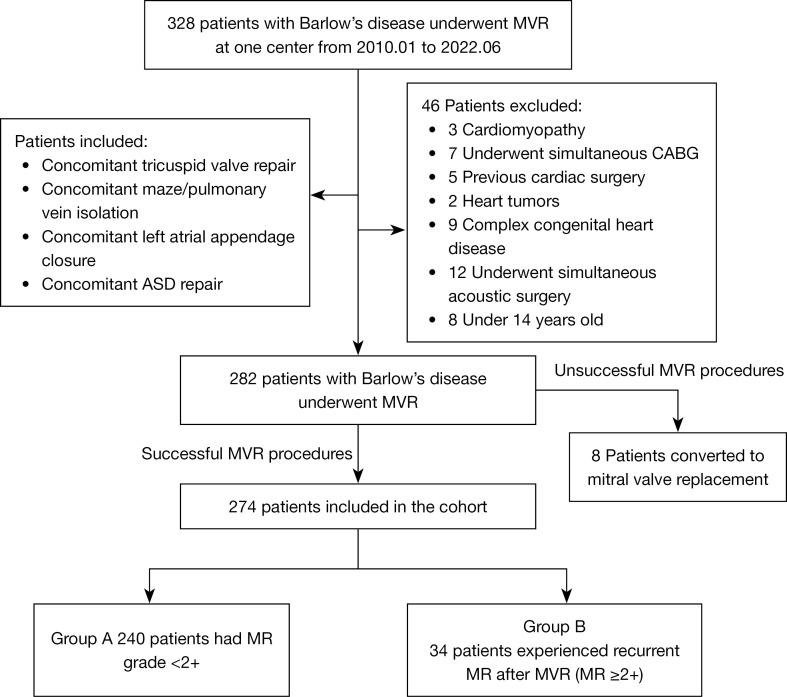
We retrospectively analyzed the clinical outcomes of 274 patients undergoing MVR for BD at a tertiary hospital (Guangdong People's Hospital, Guangzhou, China) between January 2010 and June 2022. To analyze the results of MVR and identify the risk factors for MR recurrence, we defined two groups: a total of 240 patients with MR grade <2+ (group A) and a total of 34 patients who had recurrent MR after MVR (group B; the patients with MR ≥2+). All patients were operated on using standard repair techniques. Recurrent MR was the primary outcome. Secondary outcomes were death and reoperation after MVR. Patients were followed up until March 2023. Patients were followed up by clinic visits, telephone calls, and postal or electronic questionnaires.
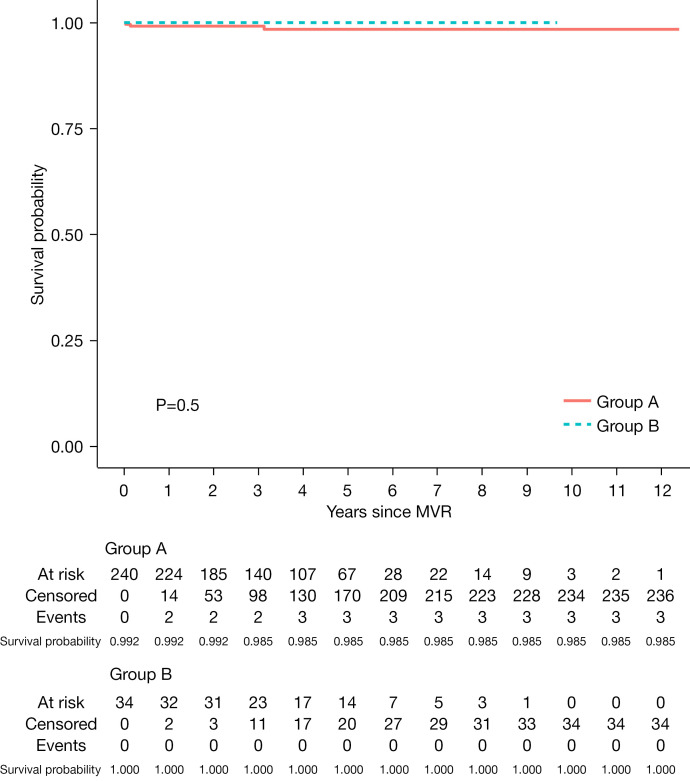
The median [range] patient age was 46.00 [16-75] years and 186 (67.9%) patients were male. Concomitant procedures were performed in 123 patients: tricuspid valve repair 71 (25.9%), maze or pulmonary vein isolation (PVI) 12 (4.4%), atrial septal defect (ASD) repair 3 (1.1%), and left atrial appendage (LAA) closure 28 (10.2%). Hospital mortality was 0.4%. Long-term complications included radiofrequency ablation in 7 patients (2.6%), pacemaker implantation in 1 patient (0.4%), and stroke in 3 patients (1.1%). The median follow-up was 3.28 (range, 0-12.39) years. Considering the competing risk of mortality, the cumulative incidence of MR progression 2+ or more grades was 2.6%, 5.9%, 14.5%, and 27.7% at 1 month, 1, 5, and 10 years, respectively. Overall survival at 1, 5, and 10 years was 99.3%, 98.6%, and 98.6%, respectively. The immediate postoperative MR area [hazard ratio (HR) =1.723; 95% confidence interval (CI): 1.051-2.824; P=0.031], postoperative left ventricular end-diastolic dimension (LVEDD) (HR =1.149; 95% CI: 1.016-1.300; P=0.027), and postoperative MR grade {HR = Exp[4.500 - 0.544 × ln(t + 20)]; P=0.008} were associated with an increased risk of MR recurrence, whereas a higher left ventricular ejection fraction (LVEF) (HR =0.931; 95% CI: 0.868-0.999; P=0.049) was associated with a decreased risk.
MVR in patients with BD can be performed with low mortality and complications and is associated with superior long-term outcomes. However, MVR was associated with a certain risk of MR recurrence, especially in those with high postoperative LVEDD, residual MR >1+, and decreased postoperative LVEF. We recommend MVR for patients with BD, especially for those with early-stage disease. However, future randomized controlled trials are needed to confirm this.
巴洛氏病(BD)是退行性二尖瓣(MV)疾病的常见病因,常导致严重的二尖瓣反流(MR)。BD的病理学对于进行二尖瓣修复(MVR)的外科医生来说具有挑战性。然而,大多数MVR有效性研究都是基于生存率和再次手术风险。本研究的目的是分析BD患者MVR的安全性、有效性和耐久性,并确定影响MR复发的因素。
我们回顾性分析了2010年1月至2022年6月期间在一家三级医院(中国广州广东省人民医院)接受BD MVR的274例患者的临床结果。为了分析MVR的结果并确定MR复发的危险因素,我们定义了两组:共有240例MR分级<2+的患者(A组)和共有34例MVR后出现MR复发的患者(B组;MR≥2+的患者)。所有患者均采用标准修复技术进行手术。MR复发是主要结局。次要结局是MVR后的死亡和再次手术。对患者进行随访直至2023年3月。通过门诊就诊、电话以及邮寄或电子问卷对患者进行随访。
患者年龄中位数[范围]为46.00[16 - 75]岁,186例(67.9%)为男性。123例患者进行了同期手术:三尖瓣修复71例(25.9%)、迷宫或肺静脉隔离(PVI)12例(4.4%)、房间隔缺损(ASD)修复3例(1.1%)以及左心耳(LAA)封堵28例(10.2%)。医院死亡率为0.4%。长期并发症包括7例患者(2.6%)进行了射频消融、1例患者(0.4%)植入了起搏器以及3例患者(1.1%)发生了卒中。中位随访时间为3.28(范围,0 - 12.39)年。考虑到死亡的竞争风险,MR进展2+或更高分级的累积发生率在1个月、1年、5年和10年时分别为2.6%、5.9%、14.5%和27.7%。1年、5年和10年时的总生存率分别为99.3%、98.6%和98.6%。术后即刻MR面积[风险比(HR)=1.723;95%置信区间(CI):1.051 - 2.824;P = 0.031]、术后左心室舒张末期内径(LVEDD)(HR = 1.149;95% CI:1.016 - 1.300;P = 0.027)以及术后MR分级{HR = Exp[4.500 - 0.544 × ln(t + 20)];P = 0.008}与MR复发风险增加相关,而较高的左心室射血分数(LVEF)(HR = 0.931;95% CI:0.868 - 0.999;P = 0.049)与风险降低相关。
BD患者的MVR可以在低死亡率和并发症的情况下进行,并且具有良好的长期结局。然而,MVR与一定的MR复发风险相关,尤其是在术后LVEDD高、残余MR>1+以及术后LVEF降低的患者中。我们建议对BD患者进行MVR,尤其是早期疾病患者。然而,需要未来的随机对照试验来证实这一点。