Bludevich Bryce, Dickson Kevin M, Reddington Hayley, Lim Chelsea Jeewoo, Hazeltine Max, Buettner Hannah, Weaver Anne, Yarzebski Jorge, Emmerick Isabel Cristina Martins, Zayaruzny Maksim, Kadiyala Mamatha, Maxfield Mark W, Uy Karl, Lou Feiran
Division of Thoracic Surgery, UMass T.H. Chan School of Medicine, Worcester, MA, USA.
Interprofessional Center for Experiential Learning and Simulation, UMass T.H. Chan School of Medicine, Worcester, MA, USA.
J Thorac Dis. 2024 Jul 30;16(7):4286-4294. doi: 10.21037/jtd-24-291. Epub 2024 Jul 18.
Although robotic surgery has gained popularity, safety concerns remain due to potential delay in addressing intraoperative hemorrhages since the surgeon is not at the bedside. This study aimed to test whether a training program for emergency robotic undocking protocols improved the performance of thoracic operating room (OR) teams.
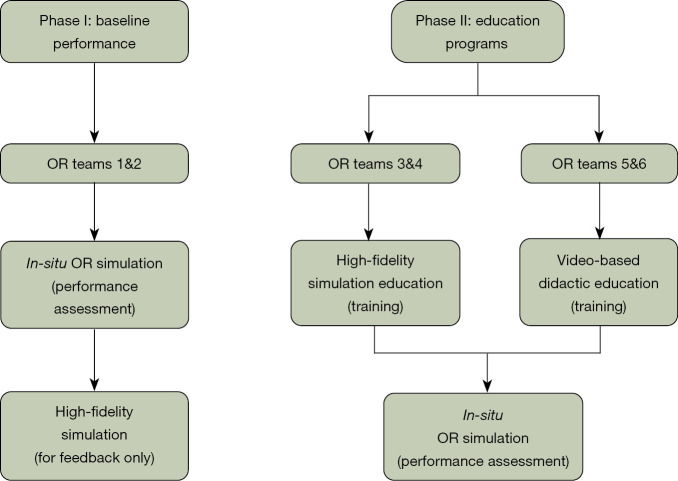
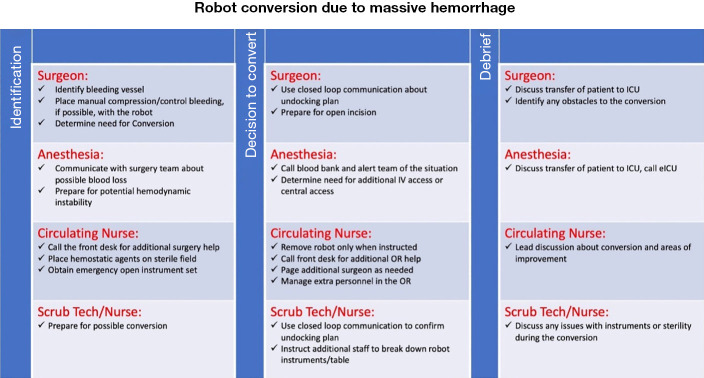
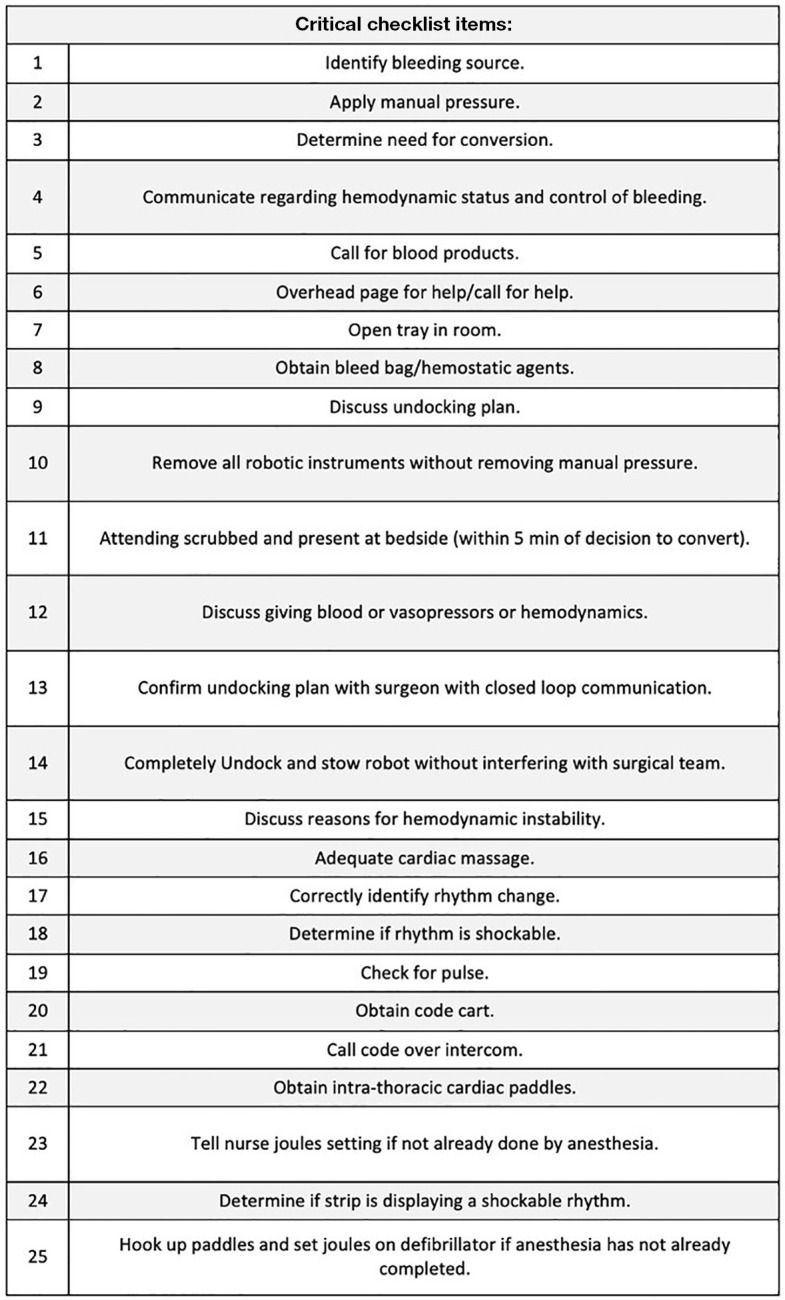
An emergency undocking protocol and checklists were created for massive hemorrhage during robotic thoracic surgery. In phase I, two OR teams participated in simulations of the scenarios in the OR without knowledge of the protocols. In phase II, the protocol and checklists were introduced to four different OR teams by either high-fidelity lab simulation or video-based didactic sessions. The teams' performances were tested with OR simulations. Performance assessments included the number of missed critical steps, participant-reported feedback, and timeliness of crucial steps.
All teams successfully converted from robot-assisted to open, with the attending at bedside within five minutes from the decision to convert, regardless of phase or education type. Phase I (control) teams had an average of 2.55 critical misses per team while the average was 0.25 for phase II teams (P=0.08). There was no significant difference between phases in time required for the surgeon to be at the bedside (average 132.2 seconds, P=0.64).
Targeted education can lead to improved team performance. This study shows that high-fidelity simulation and didactic sessions can both be used to effectively teach emergency undocking protocols.
尽管机器人手术越来越受欢迎,但由于外科医生不在床边,在处理术中出血时可能会出现延迟,因此安全问题仍然存在。本研究旨在测试紧急机器人解除对接方案的培训计划是否能提高胸外科手术室(OR)团队的表现。
针对机器人辅助胸外科手术中的大出血情况制定了紧急解除对接方案和检查表。在第一阶段,两个手术室团队在不了解方案的情况下参与了手术室场景模拟。在第二阶段,通过高保真实验室模拟或基于视频的教学课程,将方案和检查表介绍给四个不同的手术室团队。通过手术室模拟测试团队的表现。绩效评估包括遗漏的关键步骤数量、参与者报告的反馈以及关键步骤的及时性。
所有团队都成功地从机器人辅助转换为开放手术,主刀医生在决定转换后的五分钟内到达床边,无论处于哪个阶段或接受何种教育类型。第一阶段(对照组)团队平均每个团队有2.55次关键失误,而第二阶段团队的平均失误次数为0.25次(P = 0.08)。外科医生到达床边所需的时间在两个阶段之间没有显著差异(平均132.2秒,P = 0.64)。
有针对性的教育可以提高团队表现。本研究表明,高保真模拟和教学课程都可用于有效地教授紧急解除对接方案。