Zhou Wei, Liu Xiaobin, Lv Xingping, Shen Tuo, Ma Shaolin, Zhu Feng
Department of Critical Care Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, China.
J Thorac Dis. 2024 Jul 30;16(7):4495-4503. doi: 10.21037/jtd-24-242. Epub 2024 Jul 16.
Model for end-stage liver disease (MELD) is an effective predictive marker for renal, hepatic, and cardiac dysfunctions. In this study, we explore the correlation between MELD scores and the outcomes of patients undergoing cardiac valve surgery.
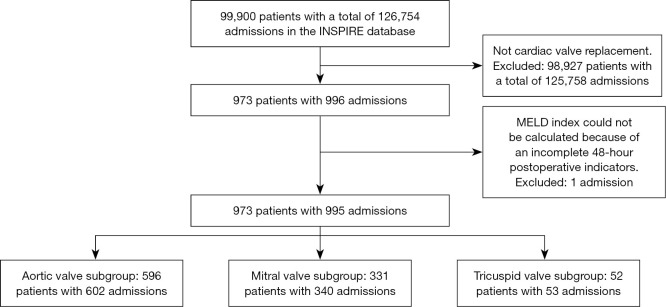
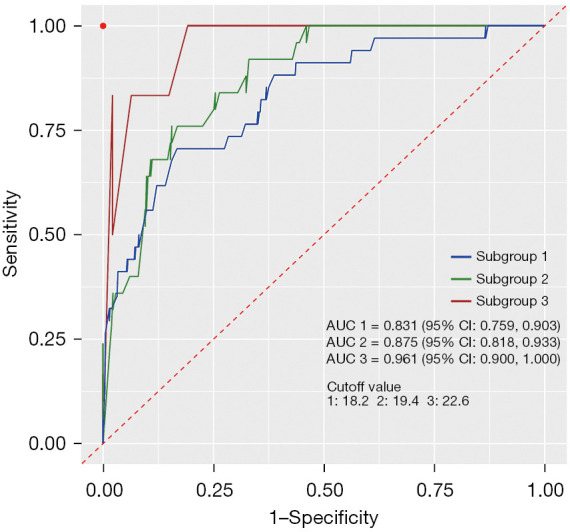
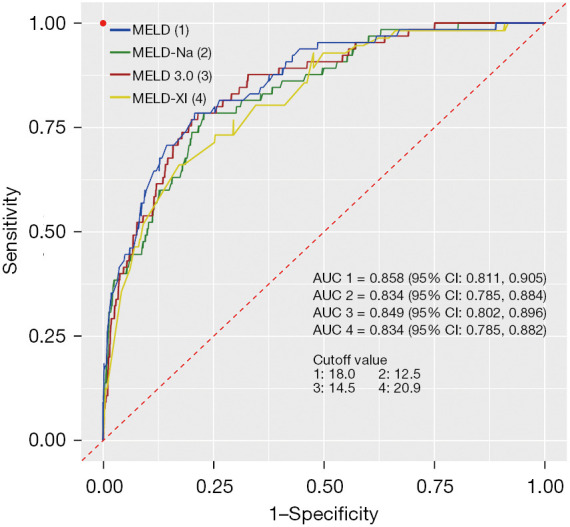
We conducted a retrospective analysis of clinical data from patients who underwent cardiac valve surgery, encompassing procedures on the aortic valve, mitral valve, and tricuspid valve, using the Informative Surgical Patient dataset for Innovative Research Environment (INSPIRE) database, we conducted receiver operating characteristic (ROC) analyses on the study participants and chose MELD as the primary scoring tool for our study due to its optimal area under the curve (AUC), patients were stratified into high (MELD ≥18) and low (MELD <18) groups based on the determined cutoff value. The perioperative clinical data of the two groups were compared.
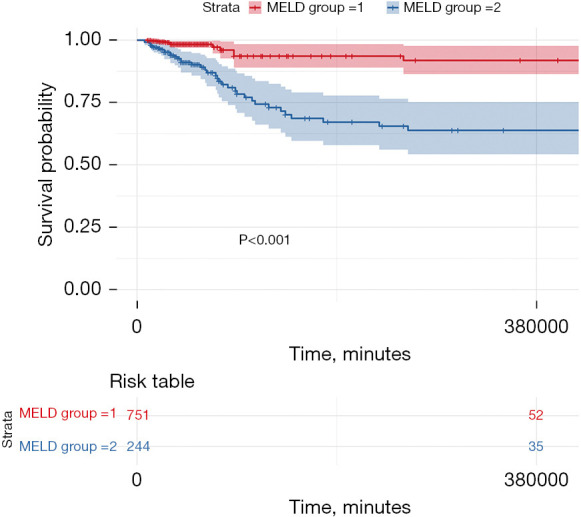
The analysis revealed 751 patients in the low MELD group (75.5%) and 244 patients (24.5%) in the high MELD group. Patients in the high MELD group exhibited a lower body mass index (BMI) compared to those in the low MELD group. In comparison to the low MELD group, the high MELD group exhibited a higher rate of emergency surgery (10.66% . 5.99%, P=0.01), along with prolonged anesthesia time, surgery time, and cardiopulmonary bypass (CPB) time. Regarding clinical prognosis, the high MELD group demonstrated a higher 28-day mortality rate (10.66% . 0.8%, P<0.001), as also observed in the analysis of three valve subgroups. Additionally, the high MELD group experienced longer hospitalization and intensive care unit (ICU) stay, and a higher proportion of patients requiring mechanical circulatory support, including intra-aortic balloon pump (IABP) assist (14.75% . 3.86%, P<0.001), extracorporeal membrane oxygenation (ECMO) assist (7.38% . 0.8%, P<0.001), and continuous renal replacement therapy (CRRT) (27.87% . 1.46%, P<0.001) post-surgery. The Kaplan-Meier survival curves illustrated a significantly lower mortality rate in the low MELD group compared to the high MELD group, with highly significant statistical differences (P<0.001).
The MELD score demonstrates a robust predictive value for clinical outcomes following cardiac valve surgery, underscoring its utility as a viable metric for disease stratification research.
终末期肝病模型(MELD)是一种用于预测肾、肝和心脏功能障碍的有效指标。在本研究中,我们探讨了MELD评分与接受心脏瓣膜手术患者预后之间的相关性。
我们对接受心脏瓣膜手术患者的临床资料进行了回顾性分析,包括主动脉瓣、二尖瓣和三尖瓣手术,使用创新研究环境信息外科患者数据集(INSPIRE)数据库,对研究参与者进行了受试者操作特征(ROC)分析,并选择MELD作为本研究的主要评分工具,因为其曲线下面积(AUC)最佳,根据确定的临界值将患者分为高(MELD≥18)和低(MELD<18)两组。比较两组的围手术期临床资料。
分析显示,低MELD组有751例患者(75.5%),高MELD组有244例患者(24.5%)。高MELD组患者的体重指数(BMI)低于低MELD组。与低MELD组相比,高MELD组的急诊手术率更高(10.66%对5.99%,P=0.01),同时麻醉时间、手术时间和体外循环(CPB)时间延长。关于临床预后,高MELD组的28天死亡率更高(10.66%对0.8%,P<0.001),在三个瓣膜亚组的分析中也观察到了这一点。此外,高MELD组的住院时间和重症监护病房(ICU)停留时间更长,需要机械循环支持的患者比例更高,包括术后主动脉内球囊泵(IABP)辅助(14.75%对3.86%,P<0.001)、体外膜肺氧合(ECMO)辅助(7.38%对0.8%,P<0.001)和持续肾脏替代治疗(CRRT)(27.87%对1.46%,P<0.001)。Kaplan-Meier生存曲线显示,低MELD组的死亡率明显低于高MELD组,差异具有高度统计学意义(P<0.001)。
MELD评分对心脏瓣膜手术后的临床结局具有强大的预测价值,强调了其作为疾病分层研究可行指标的实用性。