Chen Yiming, Dai Xiaoqing, Hu Tingting, Jiang Chen, Pan Yongmiao
Department of Prenatal Diagnosis and Screening Center, Hangzhou Women's Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou, China.
The Fourth School of Clinical Medical, Zhejiang Chinese Medical University, Hangzhou, China.
Transl Pediatr. 2024 Jul 31;13(7):1071-1085. doi: 10.21037/tp-24-58. Epub 2024 Jul 29.
Due to the incomplete standardization of the etiology and diagnostic criteria for fetal growth restriction (FGR), there has been uncertainty in the early prediction of FGR. The comprehensive estimation of FGR was mainly based on various factors, such as maternal characteristics and medical history, nuchal translucency (NT), and serum biochemical markers [pregnancy-associated plasma protein-A (PAPP-A) and free beta human chorionic gonadotropin (free β-hCG)]. Herein, we performed a retrospective cohort study to investigate the correlation and diagnostic value of maternal markers such as PAPP-A, free β-hCG, and NT in the first trimester with maternal characteristics, so as to provide theoretical basis for perinatal care and the application of low-dose aspirin.
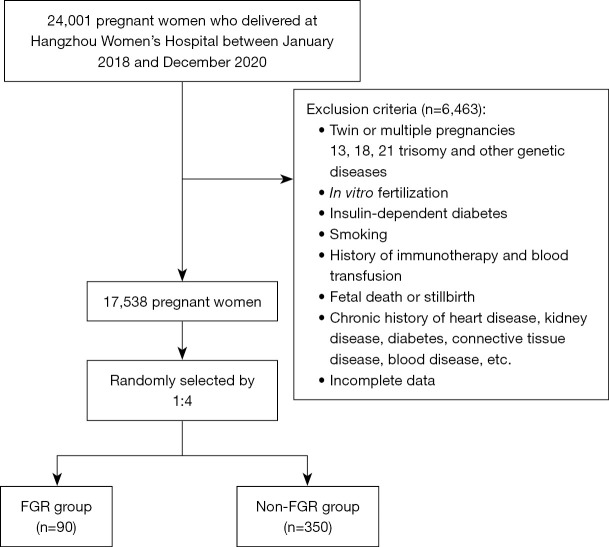
A retrospective cohort study was conducted to analyze the data of an FGR group and a non-FGR group. Chi-square test and Mann-Whitney test were used for univariate analysis of qualitative or quantitative data, respectively. Modified Poisson regression calculated the relative risk (RR) and 95% confidence interval (CI) of perinatal variables; P<0.05 was considered statistically significant.
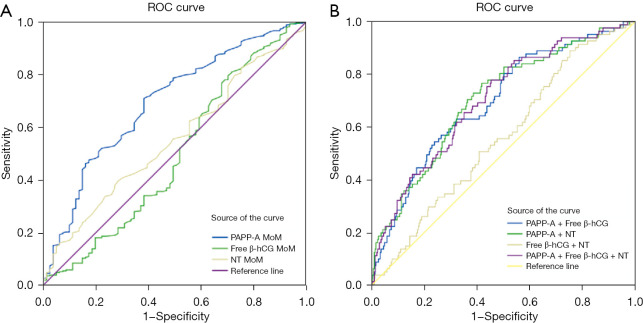
The multiple of median (MoM) of PAPP-A level and NT in the FGR group were lower than those of the non-FGR group [0.63 (0.12-2.08) 1.01 (0.28-2.41) MoM, 1.30 (0.80-2.07) 1.40 (0.80-2.20) cm, P<0.05]. The weight, score, and length of newborns in the FGR group were lower than those in the non-FGR group (all P<0.001). Modified Poisson regression analysis showed that gestational hypertension (GH) [RR =1.836 (95% CI: 1.188-2.836)], oligohydramnios [1.420 (95% CI: 1.022-1.973)], premature rupture of membranes (PROM) [0.641 (95% CI: 0.425-0.969)], female infant [1.539 (95% CI: 1.098-2.157)], low infant length [5.700 (95% CI: 3.416-9.509)], low birth weight [1.609 (95% CI: 1.012-2.559), and increased PAPP-A MoM [0.533 (95% CI: 0.369-0.769)] were associated with FGR. The cut-off value of PAPP-A + free β-hCG + NT for predicting FGR was 0.190, with a sensitivity of 0.547 and a specificity of 0.778.
Early screening markers combined with perinatal characteristics have better diagnostic value in predicting FGR and provide a scientific basis for the clinical use of low-dose aspirin to prevent FGR.
由于胎儿生长受限(FGR)的病因及诊断标准尚未完全标准化,FGR的早期预测存在不确定性。FGR的综合评估主要基于多种因素,如孕妇特征和病史、颈项透明层(NT)以及血清生化标志物[妊娠相关血浆蛋白A(PAPP-A)和游离β人绒毛膜促性腺激素(游离β-hCG)]。在此,我们进行了一项回顾性队列研究,以探讨孕早期孕妇标志物如PAPP-A、游离β-hCG和NT与孕妇特征之间的相关性及诊断价值,从而为围产期护理和低剂量阿司匹林的应用提供理论依据。
进行一项回顾性队列研究,分析FGR组和非FGR组的数据。分别采用卡方检验和曼-惠特尼检验对定性或定量数据进行单因素分析。修正泊松回归计算围产期变量的相对风险(RR)和95%置信区间(CI);P<0.05被认为具有统计学意义。
FGR组中PAPP-A水平的中位数倍数(MoM)和NT低于非FGR组[0.63(0.12 - 2.08)MoM对1.01(0.28 - 2.41)MoM,1.30(0.80 - 2.07)cm对1.40(0.80 - 2.20)cm,P<0.05]。FGR组新生儿的体重、评分和身长低于非FGR组(均P<0.001)。修正泊松回归分析显示,妊娠期高血压(GH)[RR = 1.836(95%CI:1.188 - 2.836)]、羊水过少[1.420(95%CI:1.022 - 1.973)]、胎膜早破(PROM)[0.641(95%CI:0.425 - 0.969)]、女婴[1.539(95%CI:1.098 - 2.157)]、低身长婴儿[5.700(95%CI:3.416 - 9.509)]、低出生体重[1.609(95%CI:1.012 - 2.559)]以及升高的PAPP-A MoM[0.533(95%CI:0.369 - 0.769)]与FGR相关。PAPP-A + 游离β-hCG + NT预测FGR的截断值为0.190,敏感性为0.547,特异性为0.778。
早期筛查标志物结合围产期特征在预测FGR方面具有更好的诊断价值,并为临床使用低剂量阿司匹林预防FGR提供了科学依据。