Department of Cardiology, Korea University Anam Hospital, Korea University College of Medicine, Cardiovascular Center 73, Goryeodae-Ro, Seongbuk-Gu, Seoul, 02841, Republic of Korea.
Department of Cardiology, Heart and Brain Institute, Chung-Ang University Gwang-Myeong Hospital, Chung-Ang University College of Medicine, Gwangmyeong-Si, Republic of Korea.
BMC Med. 2024 Aug 15;22(1):335. doi: 10.1186/s12916-024-03549-y.
Concomitant use of clopidogrel and proton pump inhibitor (PPI) is common, but PPI may reduce the antiplatelet effects of clopidogrel in patients undergoing percutaneous coronary intervention (PCI). We evaluated the impact of PPI use on clinical outcomes in post-PCI patients, by incorporating P2Y12 reaction unit (PRU) and CYP2C19 genotyping results.
From a multicenter registry of patients who underwent PCI with drug-eluting stent implantation and received clopidogrel-based dual antiplatelet therapy (DAPT), patients who were prescribed a PPI at the time of PCI (PPI users) were compared to those who were not (non-users). The primary outcome included all-cause death, myocardial infarction, stent thrombosis, or cerebrovascular accident at 12 months. Major bleeding (Bleeding Academic Research Consortium [BARC] types 3-5) and gastrointestinal (GI) bleeding (BARC types 3-5) were important secondary outcomes. The adjusted outcomes were compared using a 1:1 propensity-score (PS) matching and competing risk analysis.
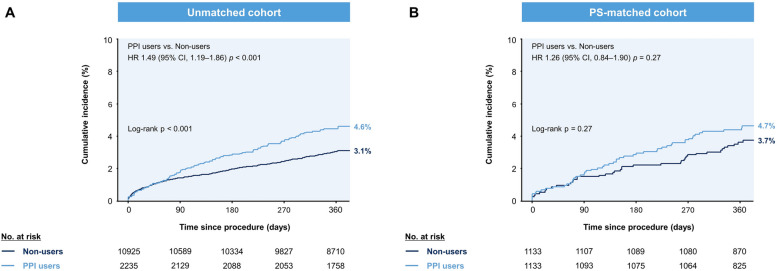
Of 13,160 patients, 2,235 (17.0%) were prescribed PPI, with an average age of 65.4 years. PPI users had higher on-treatment PRU levels than non-users. After PS matching, the primary outcome occurred in 51 patients who were PPI users (cumulative incidence, 4.7%) and 41 patients who were non-users (cumulative incidence, 3.7%; log-rank p = 0.27). In carriers of both CYP2C19 loss-of-function alleles, PPI use was linked to an increased risk of the primary outcome (hazard ratio, 3.22; 95% confidence interval, 1.18-8.78). The incidence of major bleeding and GI bleeding (BARC types 3-5) was comparable between PPI users and non-users in the PS-matched cohort.
In post-PCI patients receiving clopidogrel-based DAPT, PPI use was not linked to an increased risk of adverse cardiac and cerebrovascular events, but there was a small but significant increase in on-treatment PRU. Future research using a more individualized approach would further elucidate these interactions and guide evidence-based clinical practices.
氯吡格雷与质子泵抑制剂(PPI)同时使用较为常见,但 PPI 可能会降低行经皮冠状动脉介入治疗(PCI)患者的氯吡格雷抗血小板作用。我们通过整合 P2Y12 反应单位(PRU)和 CYP2C19 基因分型结果,评估了 PCI 后患者使用 PPI 对临床结局的影响。
从接受药物洗脱支架植入术并接受氯吡格雷双联抗血小板治疗(DAPT)的 PCI 患者多中心登记处中,比较了 PCI 时开具 PPI(PPI 使用者)与未开具 PPI(非使用者)患者的情况。主要结局包括 12 个月时全因死亡、心肌梗死、支架血栓形成或脑血管意外。主要出血(BARC 3-5 型)和胃肠道出血(BARC 3-5 型)是重要的次要结局。使用 1:1 倾向评分(PS)匹配和竞争风险分析比较调整后的结局。
在 13160 例患者中,2235 例(17.0%)开具了 PPI,平均年龄为 65.4 岁。PPI 使用者的治疗中 PRU 水平高于非使用者。经 PS 匹配后,51 例 PPI 使用者发生主要结局(累积发生率为 4.7%),41 例非使用者发生主要结局(累积发生率为 3.7%;对数秩检验 p=0.27)。在 CYP2C19 功能丧失等位基因的携带者中,PPI 使用与主要结局风险增加相关(风险比,3.22;95%置信区间,1.18-8.78)。在 PS 匹配队列中,PPI 使用者与非使用者的主要出血和胃肠道出血(BARC 3-5 型)发生率相当。
在接受氯吡格雷双联 DAPT 的 PCI 后患者中,PPI 使用与不良心脏和脑血管事件风险增加无关,但治疗中 PRU 略有升高。使用更个体化的方法进行的未来研究将进一步阐明这些相互作用,并指导基于证据的临床实践。