Department of Neurology, Jagiellonian University Medical College, Krakow, Poland.
Department of Neurology, University Hospital, Krakow, Poland.
Neuroradiology. 2024 Nov;66(11):2023-2031. doi: 10.1007/s00234-024-03443-7. Epub 2024 Aug 17.
Thrombolysis in Cerebral Infarction (TICI) 3 represents the optimal angiographic outcome following mechanical thrombectomy (MT) for acute ischemic stroke (AIS). Although it is known to yield better outcomes than TICI 2b, the influence of preprocedural cerebral hemodynamics on the clinical advantage of TICI 3 over TICI 2b remains unexplored.
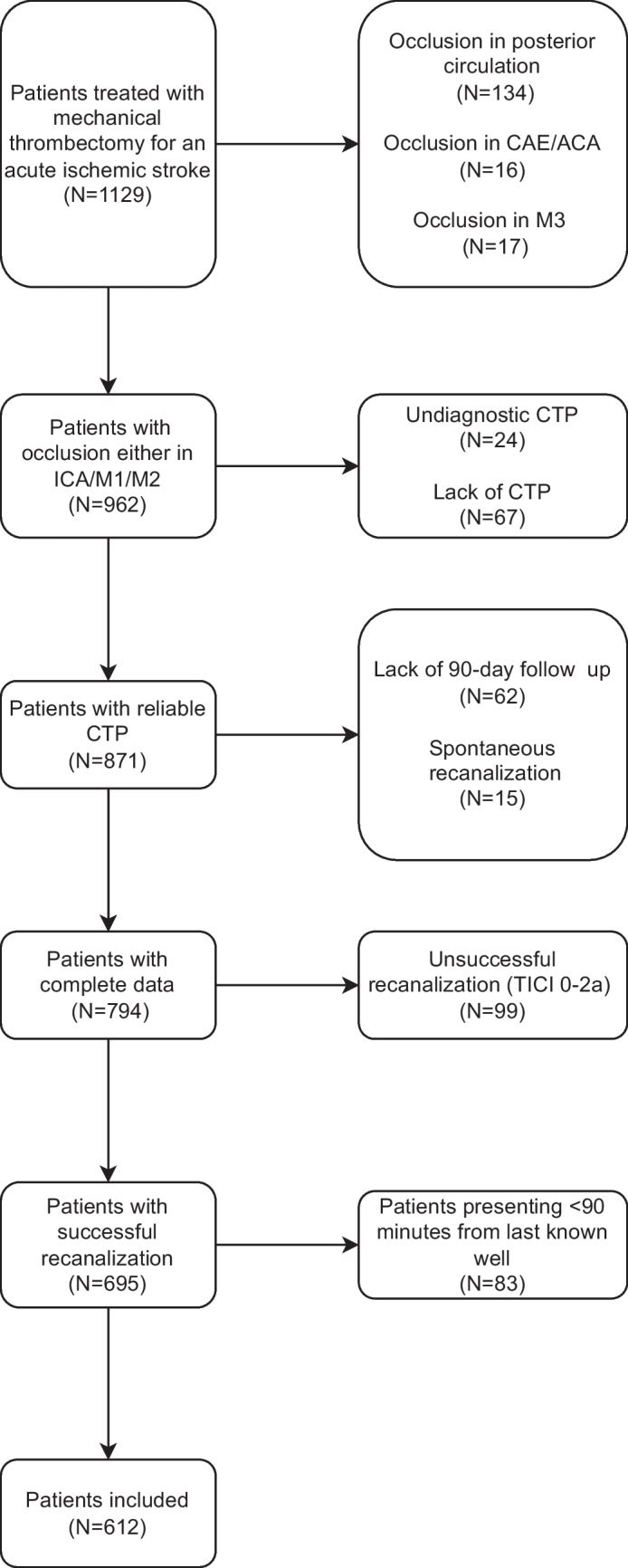
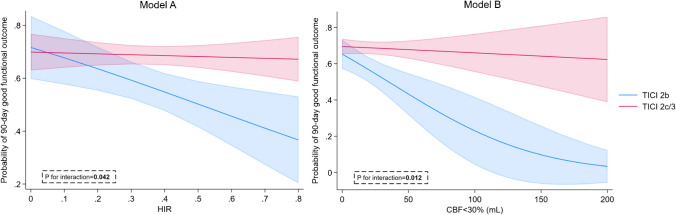
This single-center retrospective analysis involved patients with anterior circulation AIS who underwent successful recanalization during MT at the Comprehensive Stroke Center, University Hospital, Krakow between January 2019 and July 2023. We assessed the benefit of achieving TICI 2c/3 over TICI 2b on the basis of preprocedural computed perfusion imaging results, primarily focusing on early infarct volume (EIV) and tissue-level collaterals indicated by hypoperfusion intensity ratio (HIR). Good functional outcome (GFO) was defined as a modified Rankin Score < 3 on day 90.
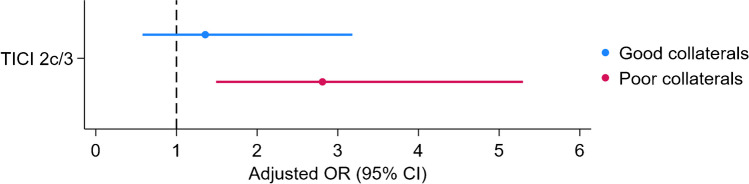
The study comprised 612 patients, of whom 467 (76.3%) achieved TICI 2c/3. GFO was more frequent in the TICI 2c/3 group (54.5% vs 69.4%, p < 0.001). There was interaction between the recanalization status and both HIR (Pi = 0.042) and EIV (Pi = 0.012) in predicting GFO, with disproportionately higher impact of HIR and EIV in TICI 2b group. The benefit from TICI 2c/3 over TICI 2b was insignificant among patients with good collaterals, defined by HIR < 0.3 (odds ratio:1.36 [0.58-3.18], p = 0.483).
TICI 2c/3 improves patient functional outcomes compared to TICI 2b regardless of EIV. However, such angiographic improvement may be clinically futile in patients with good tissue-level collateralization. Our findings suggest that preprocedural HIR should be considered when optimization of recanalization is considered during MT.
经机械取栓(MT)治疗急性缺血性脑卒中(AIS)后,血栓再通的 TICI 3 是最佳的血管造影结果。虽然它的结果优于 TICI 2b,但 TICI 3 比 TICI 2b 具有临床优势的原因仍然未知。
这是一项单中心回顾性分析,纳入了 2019 年 1 月至 2023 年 7 月在克拉科夫大学医院综合卒中中心接受 MT 成功再通的前循环 AIS 患者。我们根据术前计算灌注成像结果评估了达到 TICI 2c/3 比 TICI 2b 的获益,主要关注早期梗死体积(EIV)和低灌注强度比(HIR)表示的组织水平侧支循环。良好的功能结局(GFO)定义为第 90 天改良 Rankin 评分<3。
该研究共纳入 612 例患者,其中 467 例(76.3%)达到 TICI 2c/3。TICI 2c/3 组的 GFO 更常见(54.5% vs 69.4%,p<0.001)。再通状态与 HIR(Pi=0.042)和 EIV(Pi=0.012)在预测 GFO 方面存在交互作用,HIR 和 EIV 在 TICI 2b 组的影响不成比例地更大。在 HIR<0.3 定义的侧支循环良好的患者中,TICI 2c/3 与 TICI 2b 相比获益不显著(优势比:1.36[0.58-3.18],p=0.483)。
与 TICI 2b 相比,TICI 2c/3 改善了患者的功能结局,无论 EIV 如何。然而,在组织水平侧支循环良好的患者中,这种血管造影改善可能在临床上是无益的。我们的研究结果表明,在考虑 MT 再通优化时,应考虑术前 HIR。