Department of Infectious Disease, Imperial College London, London, UK.
Peter Medawar Building for Pathogen Research, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom.
J Int AIDS Soc. 2024 Aug;27(8):e26349. doi: 10.1002/jia2.26349.
To assess the effectiveness of novel HIV curative strategies, "cure" trials require periods of closely monitored antiretroviral therapy (ART) analytical treatment interruptions (ATIs). We performed a systematic review and meta-analysis to identify the impact of ATI with or without novel therapeutics in cure-related studies on the time to viral re-suppression following ART restart.
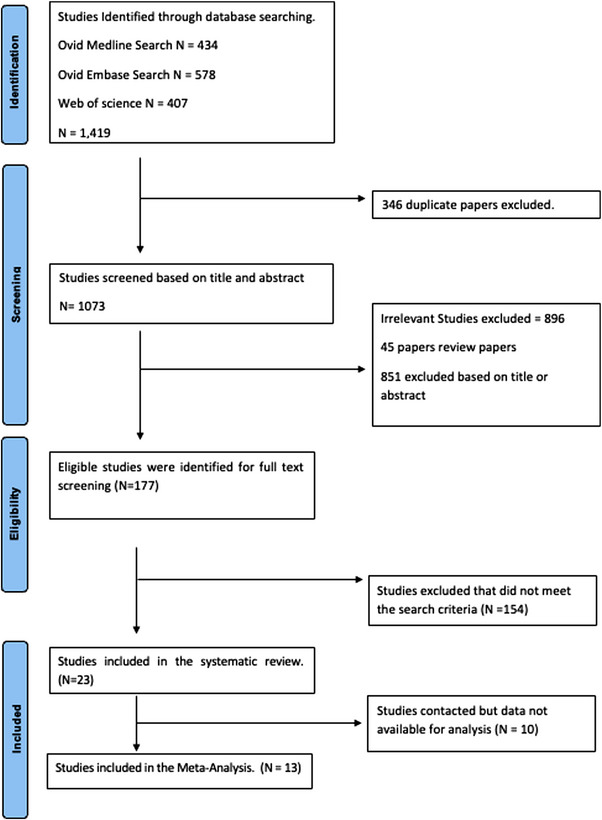
Medline, Embase and Web of Science databases were searched for human studies involving ATIs from 1 January 2015 till 22 April 2024. The primary outcome was time to first viral re-suppression (plasma HIV viral load [VL] <50 copies/ml) stratified by receipt of interventional drug with ATI (IA) or ATI-only groups. Random-effects proportional meta-analysis and multivariable Cox proportional hazards analysis were performed using R.
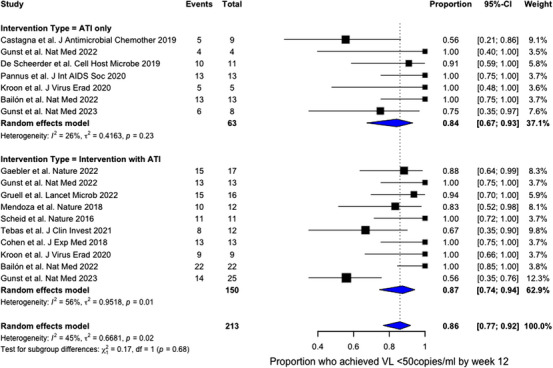
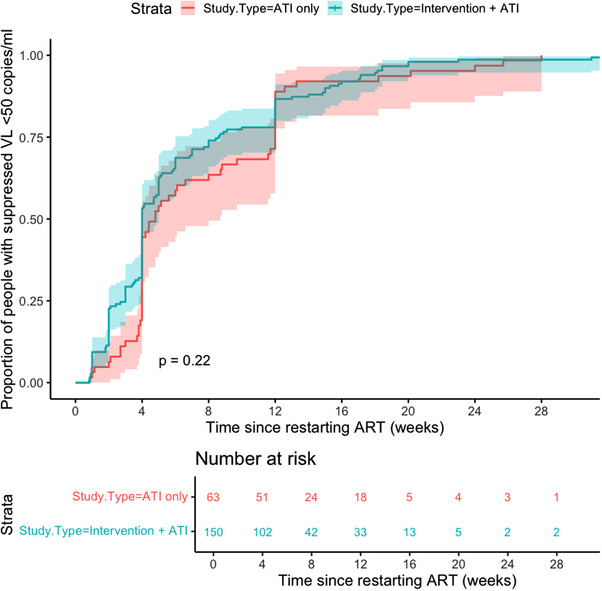
Of 1073 studies screened, 13 were included that met the inclusion criteria with VL data available after restarting ART (n = 213 participants). There was no difference between time to viral suppression in IA or ATI-only cohorts (p = 0.22). For 87% of participants, viral suppression within 12 weeks of ART restart was achieved, and all eventually had at least one VL <50 copies/ml during follow-up. After adjusting for covariables, while participants in the IA cohort were associated with less rapid suppression (adjusted hazard ratio [aHR] 0.61, 95% CI 0.40-0.94, p = 0.026), other factors include greater log VL at ART restart (aHR 0.56, 95% CI 0.46-0.68, p<0.001), duration since HIV diagnosis (aHR 0.93, 95% CI 0.89-0.96) and longer intervals between HIV VL monitoring (aHR 0.66, 95% CI 0.59-0.74, p<0.001). However, the use of integrase inhibitors was associated with more rapid viral suppression (aHR 1.74, 95% CI 1.16-2.59).
When designing studies involving ATIs, information on time to viral re-suppression after restarting ART is important to share with participants, and should be regularly monitored and reported, to assess the impact and safety of specific trial interventions in ATI studies.
The majority of participants achieved viral suppression after restarting ART in ATI studies. ART regimens containing integrase inhibitors and frequent VL monitoring should be offered for people restarting ART after ATI studies to ensure rapid re-suppression.
为了评估新型 HIV 治愈策略的有效性,“治愈”试验需要进行密切监测抗逆转录病毒治疗 (ART) 分析性治疗中断 (ATI) 的阶段。我们进行了系统评价和荟萃分析,以确定在与治愈相关的研究中,ATI 联合或不联合新型治疗药物对 ART 重启后病毒再次抑制的时间的影响。
从 2015 年 1 月 1 日至 2024 年 4 月 22 日,在 Medline、Embase 和 Web of Science 数据库中搜索涉及 ATI 的人类研究。主要结局是根据接受干预性药物治疗(IA)或仅接受 ATI 组的情况,首次病毒再次抑制(血浆 HIV 病毒载量 [VL] <50 拷贝/ml)的时间。使用 R 进行随机效应比例荟萃分析和多变量 Cox 比例风险分析。
在筛选出的 1073 项研究中,有 13 项符合纳入标准,并且在重新开始 ART 后有可用的 VL 数据(n = 213 名参与者)。IA 组或仅接受 ATI 组之间的病毒抑制时间无差异(p = 0.22)。87%的参与者在 ART 重启后 12 周内实现了病毒抑制,所有参与者最终在随访期间至少有一次 VL <50 拷贝/ml。在调整协变量后,IA 组的参与者与更快的抑制相关(调整后的危险比[aHR] 0.61,95%CI 0.40-0.94,p = 0.026),其他因素包括在 ART 重启时更大的 log VL(aHR 0.56,95%CI 0.46-0.68,p<0.001)、从 HIV 诊断到开始 ART 的时间(aHR 0.93,95%CI 0.89-0.96)和 HIV VL 监测间隔较长(aHR 0.66,95%CI 0.59-0.74,p<0.001)。然而,使用整合酶抑制剂与更快的病毒抑制相关(aHR 1.74,95%CI 1.16-2.59)。
在设计涉及 ATI 的研究时,提供关于重新开始 ART 后病毒再次抑制时间的信息对参与者很重要,并且应定期监测和报告,以评估特定试验干预措施在 ATI 研究中的影响和安全性。
大多数参与者在 ATI 研究中重新开始 ART 后实现了病毒抑制。在 ATI 研究后重新开始 ART 时,应提供包含整合酶抑制剂和频繁 VL 监测的 ART 方案,以确保快速抑制。