Goichot Bernard, Lefebvre François, Vinzio Stéphane, Cailleux Anne, Kuhn Jean-Marc, Schneegans Olivier, Catargi Bodgan, Gilly Olivier, Baltzinger Philippe, Meyer Nicolas, Caron Philippe
B Goichot, Department of Endocrinology, Diabetology and Nutrition, Strasbourg University Hospital, Strasbourg, France.
F Lefebvre, Strasbourg University Hospital, Strasbourg, France.
Eur Thyroid J. 2024 Aug 1;13(6). doi: 10.1530/ETJ-24-0121.
Subclinical hyperthyroidism (SCH) is common and associated with atrial fibrillation (AF) risk in the elderly. Current guidelines rely on a low level of evidence.
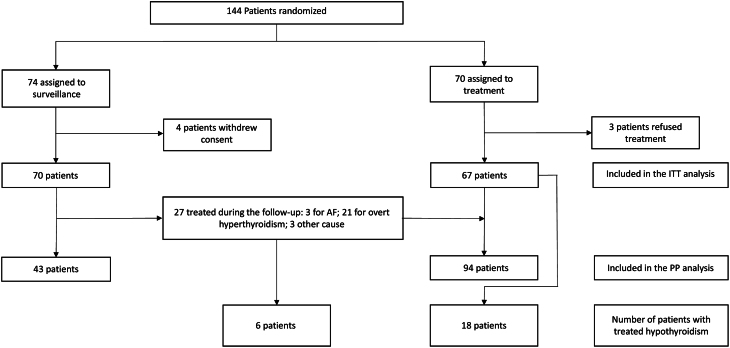
Randomized clinical trial including patients 50 years and older, with TSH <0.4 mU/L and normal thyroid hormone concentrations. All patients showed autonomy on thyroid scan. They were randomized either to receive radioiodine (I131) or to be monitored and treated only if they underwent AF or evolved towards overt hyperthyroidism. Primary outcome was the onset of new AF. Secondary outcomes were treatment-induced hypothyroidism rate and health-related quality of life.
144 patients (mean age 65.3±8.9y, 76% female) were randomized, 74 to surveillance and 70 to treatment. Four patients in the surveillance group and one in the treatment group developed AF (p=0.238). However, the patient who developed AF in the treatment group maintained TSH <0.4 mU/L at AF onset. A post-hoc analysis was carried out and showed that when normalization of TSH was considered, the risk of AF was significantly reduced (p=0.0003). In the surveillance group, several patients showed no classical characteristics associated with AF risk, including age>65y or TSH<0.1mU/L. Of 94 patients treated using radioiodine, 25% developed hypothyroidism during follow-up.
Due to recruitment difficulties this study failed to demonstrate that SCH treatment can reduce significantly the incidence of AF in patients older than 50 years with thyroid autonomy even if all the patients who developed AF maintained TSH <0.4 mU/L. This result must be balanced with the increased risk of radioiodine-induced hypothyroidism.
亚临床甲状腺功能亢进症(SCH)很常见,且与老年人房颤(AF)风险相关。当前指南所依据的证据水平较低。
一项随机临床试验,纳入年龄在50岁及以上、促甲状腺激素(TSH)<0.4 mU/L且甲状腺激素浓度正常的患者。所有患者甲状腺扫描显示有自主性。他们被随机分为接受放射性碘(I131)治疗组或仅在发生房颤或发展为显性甲状腺功能亢进症时才进行监测和治疗组。主要结局是新发房颤的发生。次要结局是治疗引起的甲状腺功能减退症发生率和健康相关生活质量。
144例患者(平均年龄65.3±8.9岁,76%为女性)被随机分组,74例接受监测,70例接受治疗。监测组有4例患者和治疗组有1例患者发生房颤(p = 0.238)。然而,治疗组中发生房颤的患者在房颤发作时TSH仍<0.4 mU/L。进行了一项事后分析,结果显示,当考虑TSH正常化时,房颤风险显著降低(p = 0.0003)。在监测组中,有几位患者没有显示出与房颤风险相关的典型特征,包括年龄>65岁或TSH<0.1 mU/L。在94例接受放射性碘治疗的患者中,25%在随访期间发生了甲状腺功能减退症。
由于招募困难,本研究未能证明对50岁以上有甲状腺自主性的患者进行SCH治疗能显著降低房颤发生率,即使所有发生房颤的患者TSH仍<0.4 mU/L。这一结果必须与放射性碘诱发甲状腺功能减退症风险增加相权衡。