Clinical Pharmacology and Quantitative Pharmacology, Clinical Pharmacology and Safety Science, R&D, AstraZeneca, Cambridge, UK.
Certara, Radnor, Pennsylvania, USA.
Br J Clin Pharmacol. 2024 Dec;90(12):3263-3276. doi: 10.1111/bcp.16199. Epub 2024 Aug 19.
Osimertinib is a third-generation, irreversible, central nervous system-active, epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI) with efficacy in EGFR-mutated non-small cell lung cancer (NSCLC). We assessed the relationship between plasma osimertinib levels and its efficacy and safety events.
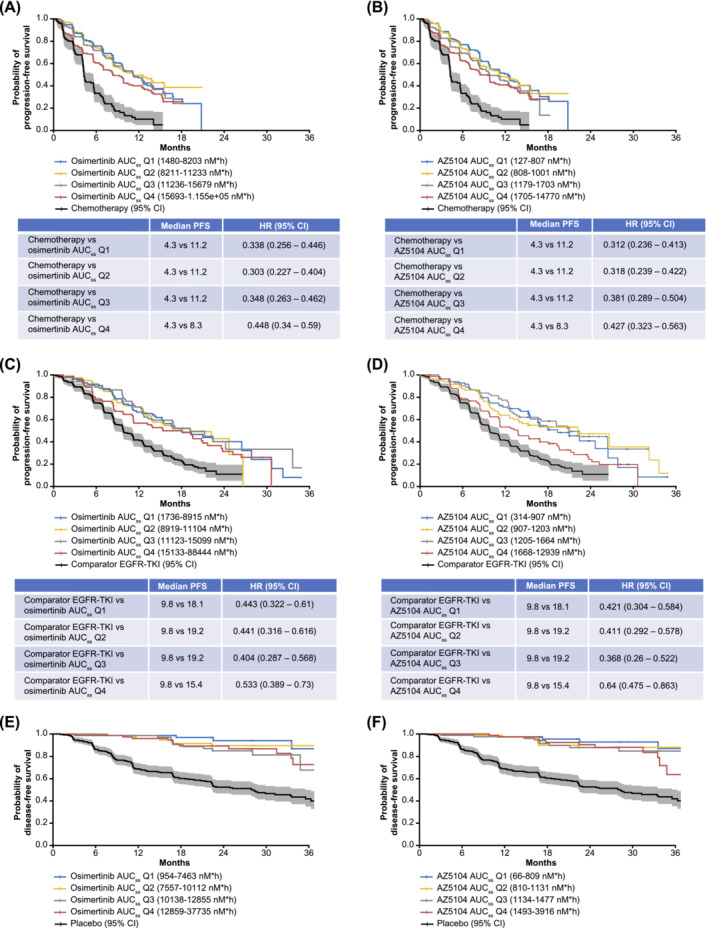
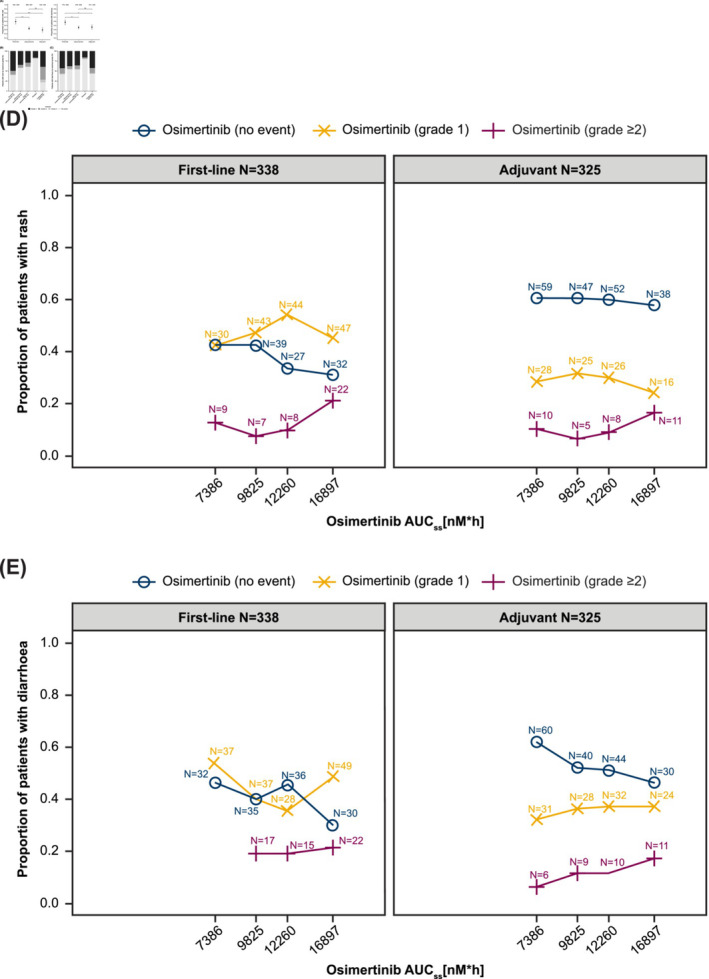
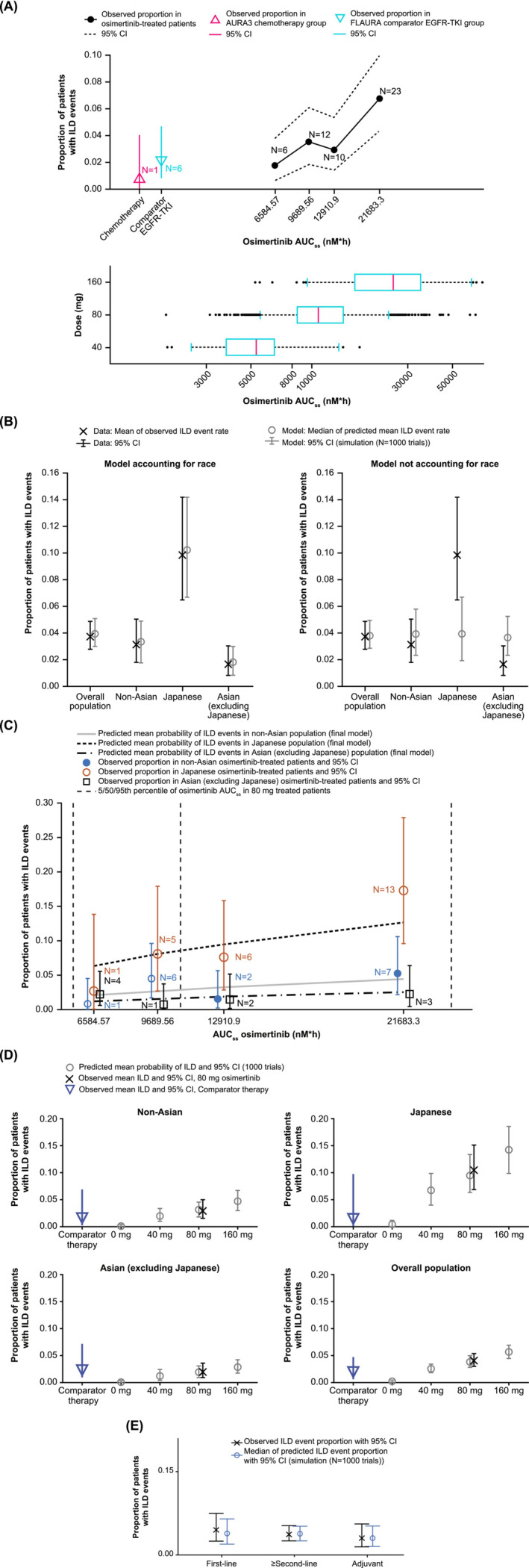
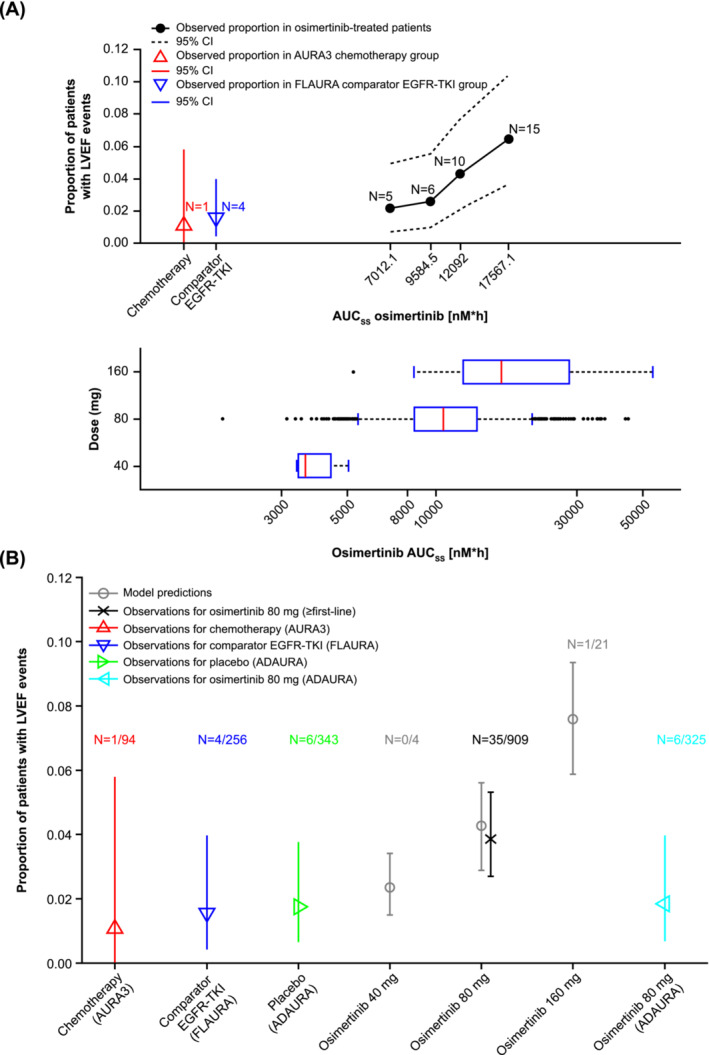
Comprehensive pharmacokinetics exposure-response (E-R) modelling was performed utilizing steady state area under the curve (AUC) data from first-line, ≥second-line and adjuvant studies from the osimertinib clinical development programme (20-240 mg once-daily dosing; N = 1689 patients). Analyses were conducted for survival using a proportional hazard model; for interstitial lung disease (ILD) and left ventricular ejection fraction (LVEF) events using a penalized logistic regression model and graphical analysis of potential confounding factors; and for rash and diarrhoea events using descriptive analysis.
E-R modelling analyses indicated no clear trend of increasing efficacy with increasing osimertinib AUC; efficacy in all exposure quartiles was significantly better than the control arm (comparator EGFR-TKI, chemotherapy or placebo) irrespective of treatment line. Model-based analysis suggested a potential relationship between increased osimertinib exposure and increased probability of ILD events, predominantly in Japanese patients. Additionally, there were increased probabilities of rash or diarrhoea with increasing osimertinib exposure. The probability of LVEF events showed overlapping confidence intervals for osimertinib ≤80 mg and control.
E-R modelling in patients with EGFR-mutated NSCLC demonstrated that increased osimertinib exposure was unlikely to increase efficacy but may increase occurrence of certain adverse events. Hence, long-term treatment with doses ≥80 mg was not expected to provide additional benefit.
奥希替尼是第三代、不可逆、中枢神经系统活性的表皮生长因子受体(EGFR)酪氨酸激酶抑制剂(TKI),对 EGFR 突变型非小细胞肺癌(NSCLC)有效。我们评估了血浆奥希替尼水平与其疗效和安全性事件之间的关系。
利用奥希替尼临床开发项目(20-240mg 每日一次剂量)一线、≥二线和辅助研究中的稳态 AUC 数据,对全面的药代动力学暴露-反应(E-R)模型进行了综合评估(N=1689 例患者)。使用比例风险模型对生存进行分析;使用惩罚逻辑回归模型和潜在混杂因素的图形分析对间质性肺病(ILD)和左心室射血分数(LVEF)事件进行分析;使用描述性分析对皮疹和腹泻事件进行分析。
E-R 模型分析表明,随着奥希替尼 AUC 的增加,疗效没有明显的趋势;所有暴露四分位数的疗效均显著优于对照组(对照 EGFR-TKI、化疗或安慰剂),无论治疗线如何。基于模型的分析表明,奥希替尼暴露增加与 ILD 事件的发生概率增加之间存在潜在关系,主要发生在日本患者中。此外,奥希替尼暴露增加会增加皮疹或腹泻的发生概率。奥希替尼≤80mg 和对照的 LVEF 事件的概率置信区间重叠。
在 EGFR 突变型 NSCLC 患者中进行的 E-R 模型分析表明,奥希替尼暴露增加不太可能增加疗效,但可能会增加某些不良反应的发生。因此,预计长期使用≥80mg 的剂量不会带来额外的益处。