Beijing University of Chinese Medicine, Beijing, China.
Beijing University of Chinese Medicine Affiliated Shenzhen Hospital, Shenzhen, China.
BMC Cancer. 2024 Aug 19;24(1):1023. doi: 10.1186/s12885-024-12780-y.
The selection of appropriate second-line therapy for liver cancer after first-line treatment failure poses a significant clinical challenge due to the lack of direct comparative studies and standard treatment protocols. A network meta-analysis (NMA) provides a robust method to systematically evaluate the clinical outcomes and adverse effects of various second-line treatments for hepatocellular carcinoma (HCC).
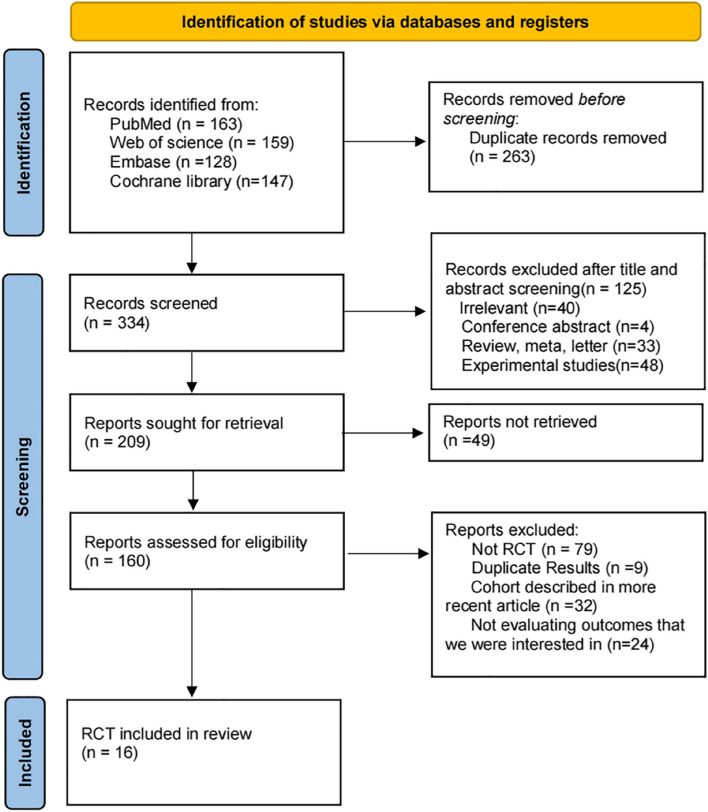
We systematically searched PubMed, Embase, Web of Science and the Cochrane Library to identify phase III/IV randomized controlled trials (RCTs) published up to March 11, 2024. The outcomes extracted were median overall survival (OS), median progression-free survival (PFS), time to disease progression (TTP), disease control rate (DCR), objective response rate (ORR), and adverse reactions. This study was registered in the Prospective Register of Systematic Reviews (CRD42023427843) to ensure transparency, novelty, and reliability.
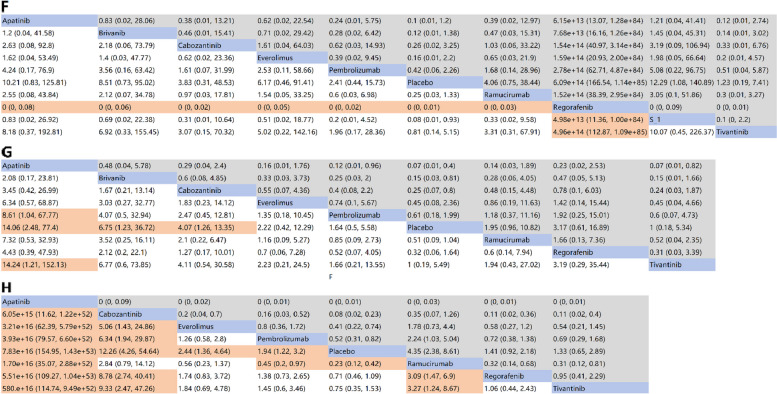
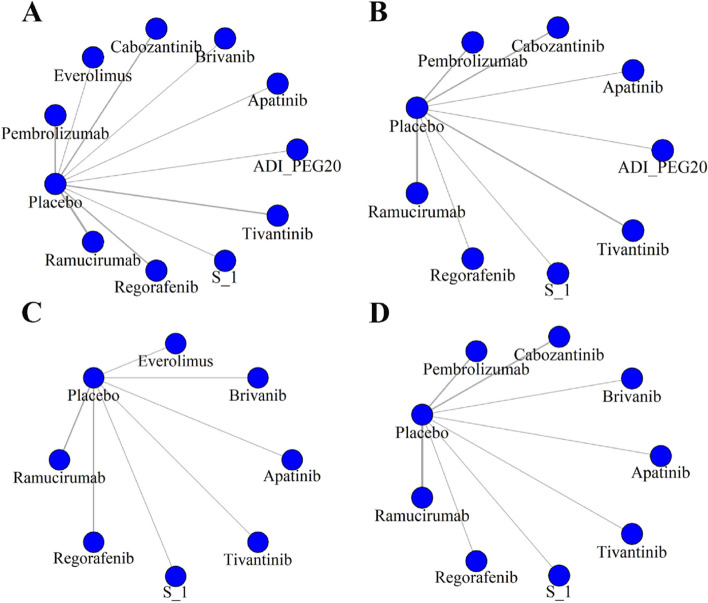
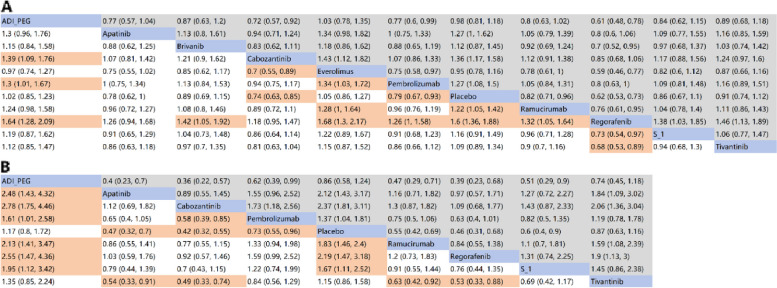
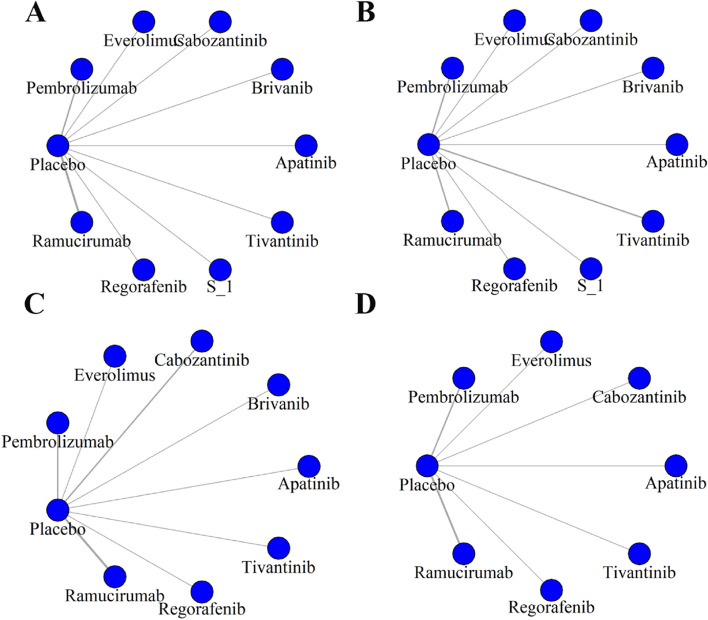
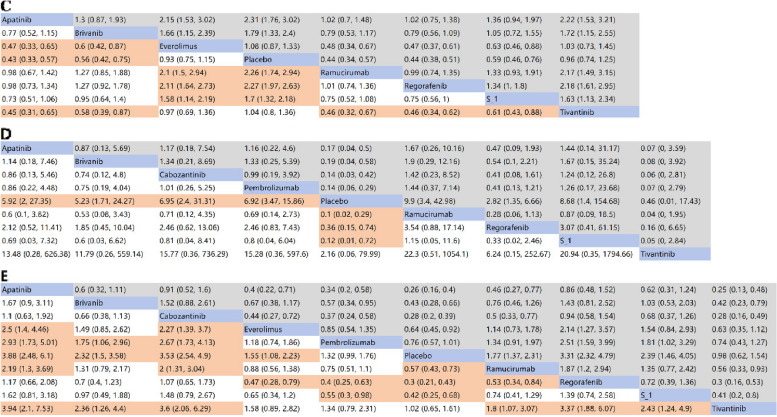
We included 16 RCTs involving 7,005 patients and 10 second-line treatments. For advanced HCC patients, regorafenib (HR = 0.62, 95%CI: 0.53-0.73) and cabozantinib (HR = 0.74, 95%CI: 0.63-0.85) provided the best OS benefits compared to placebo. Cabozantinib (HR = 0.42, 95%CI: 0.32-0.55) and regorafenib (HR = 0.46, 95% CI: 0.31-0.68) also offered the most significant PFS benefits. For TTP, apatinib (HR = 0.43, 95% CI: 0.33-0.57), ramucirumab (HR = 0.44, 95% CI: 0.34-0.57), and regorafenib (HR = 0.44, 95% CI: 0.38-0.51) showed significant benefits over placebo. Regarding ORR, ramucirumab (OR = 9.90, 95% CI: 3.40-42.98) and S-1 (OR = 8.68, 95% CI: 1.4-154.68) showed the most significant increases over placebo. Apatinib (OR = 3.88, 95% CI: 2.48-6.10) and cabozantinib (OR = 3.53, 95% CI: 2.54-4.90) provided the best DCR benefits compared to placebo. Tivantinib showed the most significant advantages in terms of three different safety outcome measures.
Our findings suggest that, in terms of overall efficacy and safety, regorafenib and cabozantinib are the optimal second-line treatment options for patients with advanced HCC.
由于缺乏直接比较研究和标准治疗方案,一线治疗失败后肝癌的二线治疗选择仍然是一个重大的临床挑战。网络荟萃分析(NMA)提供了一种强大的方法,可以系统地评估各种肝癌二线治疗的临床结局和不良反应。
我们系统地检索了 PubMed、Embase、Web of Science 和 Cochrane Library,以确定截至 2024 年 3 月 11 日发表的 III/IV 期随机对照试验(RCT)。提取的结局包括中位总生存期(OS)、中位无进展生存期(PFS)、疾病进展时间(TTP)、疾病控制率(DCR)、客观缓解率(ORR)和不良反应。本研究在系统评价前瞻性注册库(CRD42023427843)中进行了注册,以确保透明度、新颖性和可靠性。
我们纳入了 16 项 RCT,涉及 7005 名患者和 10 种二线治疗方法。对于晚期 HCC 患者,与安慰剂相比,regorafenib(HR=0.62,95%CI:0.53-0.73)和 cabozantinib(HR=0.74,95%CI:0.63-0.85)提供了最佳的 OS 获益。卡博替尼(HR=0.42,95%CI:0.32-0.55)和regorafenib(HR=0.46,95%CI:0.31-0.68)也提供了最显著的 PFS 获益。对于 TTP,阿帕替尼(HR=0.43,95%CI:0.33-0.57)、ramucirumab(HR=0.44,95%CI:0.34-0.57)和regorafenib(HR=0.44,95%CI:0.38-0.51)与安慰剂相比具有显著获益。关于 ORR,ramucirumab(OR=9.90,95%CI:3.40-42.98)和 S-1(OR=8.68,95%CI:1.4-154.68)与安慰剂相比显示出最显著的增加。阿帕替尼(OR=3.88,95%CI:2.48-6.10)和卡博替尼(OR=3.53,95%CI:2.54-4.90)与安慰剂相比提供了最佳的 DCR 获益。替伐替尼在三种不同的安全性测量指标中显示出最显著的优势。
我们的研究结果表明,在总体疗效和安全性方面,regorafenib 和卡博替尼是晚期 HCC 患者的最佳二线治疗选择。