Joosse Huibert-Jan, Groenestege Wouter Tiel, Vernooij Robin Wm, De Groot Mark Ch, Hoefer Imo E, van Solinge Wouter W, Kok Maarten B, Haitjema Saskia
Central Diagnostic Laboratory, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Department of Nephrology and Hypertension, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Digit Health. 2024 Aug 18;10:20552076241271767. doi: 10.1177/20552076241271767. eCollection 2024 Jan-Dec.
Acute kidney injury (AKI) is easily missed and underdiagnosed in routine clinical care. Timely AKI management is important to decrease morbidity and mortality risks. We recently implemented an AKI e-alert at the University Medical Center Utrecht, comparing plasma creatinine concentrations with historical creatinine baselines, thereby identifying patients with AKI. This alert is limited to data from tertiary care, and primary care data can increase diagnostic accuracy for AKI. We assessed the added value of linking primary care data to tertiary care data, in terms of timely diagnosis or excluding AKI.
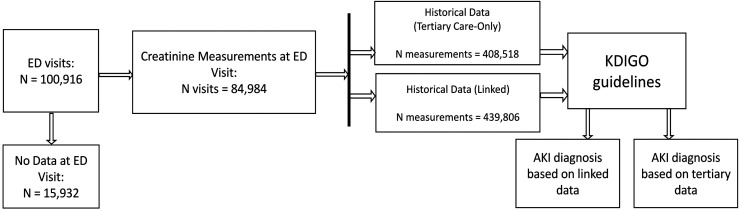
With plasma creatinine tests for 84,984 emergency department (ED) visits, we applied the Kidney Disease Improving Global Outcome guidelines in both tertiary care-only data and linked data and compared AKI cases.
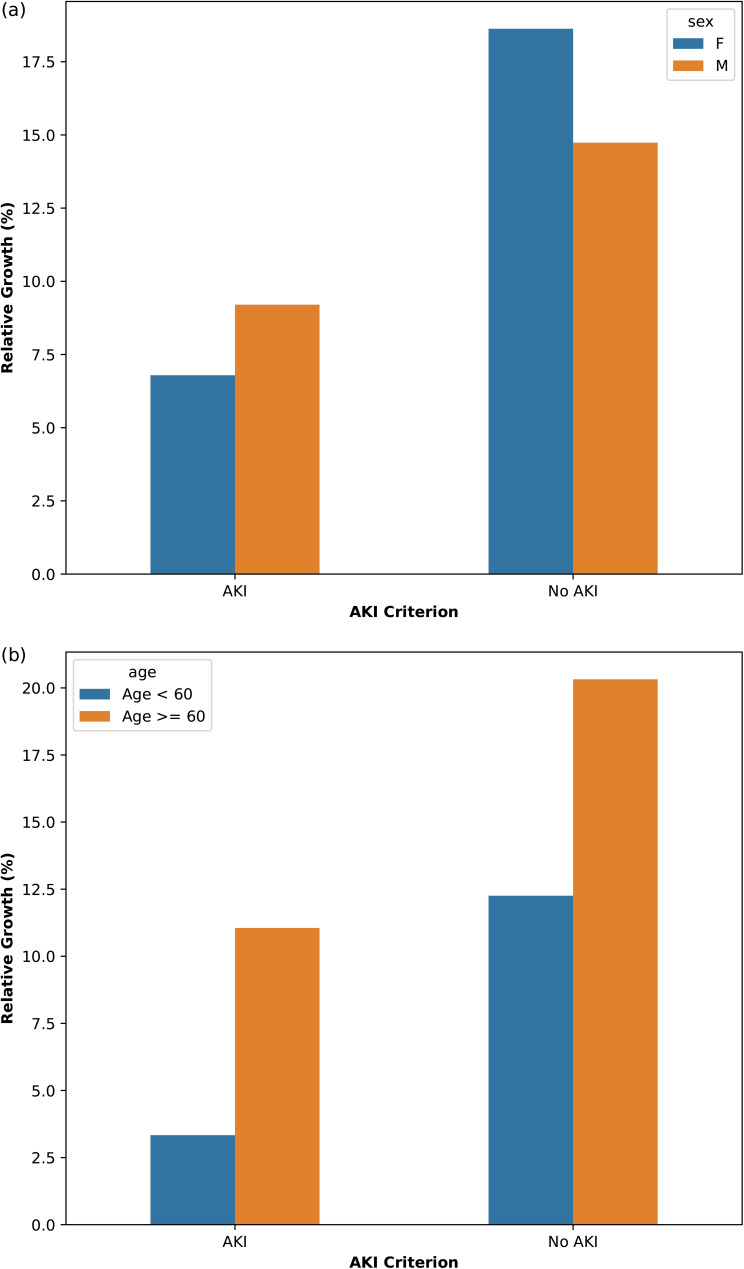
Using linked data, the presence of AKI could be evaluated in an additional 7886 ED visits. Sex- and age-stratified analyses identified the largest added value for women (an increase of 4095 possible diagnoses) and patients ≥60 years (an increase of 5190 possible diagnoses). We observed 398 additional visits where AKI was diagnosed, as well as 185 cases where AKI could be excluded. We observed no overall decrease in time between baseline and AKI diagnosis (28.4 days vs. 28.0 days). For cases where AKI was diagnosed in both data sets, we observed a decrease of 2.8 days after linkage, indicating a timelier diagnosis of AKI.
Combining primary and tertiary care data improves AKI diagnostic accuracy in routine clinical care and enables timelier AKI diagnosis.
在常规临床护理中,急性肾损伤(AKI)很容易被漏诊和诊断不足。及时管理AKI对于降低发病和死亡风险很重要。我们最近在乌得勒支大学医学中心实施了一项AKI电子警报,将血浆肌酐浓度与历史肌酐基线进行比较,从而识别出患有AKI的患者。该警报仅限于三级护理数据,而初级护理数据可以提高AKI的诊断准确性。我们评估了将初级护理数据与三级护理数据相联系在及时诊断或排除AKI方面的附加价值。
对于84984次急诊科就诊的血浆肌酐检测,我们在仅三级护理数据和关联数据中均应用了改善全球肾脏病预后组织的指南,并比较了AKI病例。
使用关联数据,在另外7886次急诊科就诊中可以评估AKI的存在情况。按性别和年龄分层分析发现,女性(可能诊断增加4095例)和60岁及以上患者(可能诊断增加5190例)的附加价值最大。我们观察到另外398次就诊被诊断为AKI,以及185例可以排除AKI的病例。我们观察到基线到AKI诊断之间的时间没有总体减少(28.4天对28.0天)。对于在两个数据集中均被诊断为AKI的病例,关联后我们观察到时间减少了2.8天,这表明对AKI的诊断更及时。
结合初级和三级护理数据可提高常规临床护理中AKI的诊断准确性,并能更及时地诊断AKI。