Department of Renal Medicine, University Hospitals Birmingham NHS Foundation Trust, Birmingham, B15 2GW, UK.
Department of Nephrology, Hippokration Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Biol Sex Differ. 2021 Apr 8;12(1):30. doi: 10.1186/s13293-021-00373-4.
The association of several comorbidities, including diabetes mellitus, hypertension, cardiovascular disease, heart failure and chronic kidney or liver disease, with acute kidney injury (AKI) is well established. Evidence on the effect of sex and socioeconomic factors are scarce. This study was designed to examine the association of sex and socioeconomic factors with AKI and AKI-related mortality and further to evaluate the additional relationship with other possible risk factors for AKI occurrence.
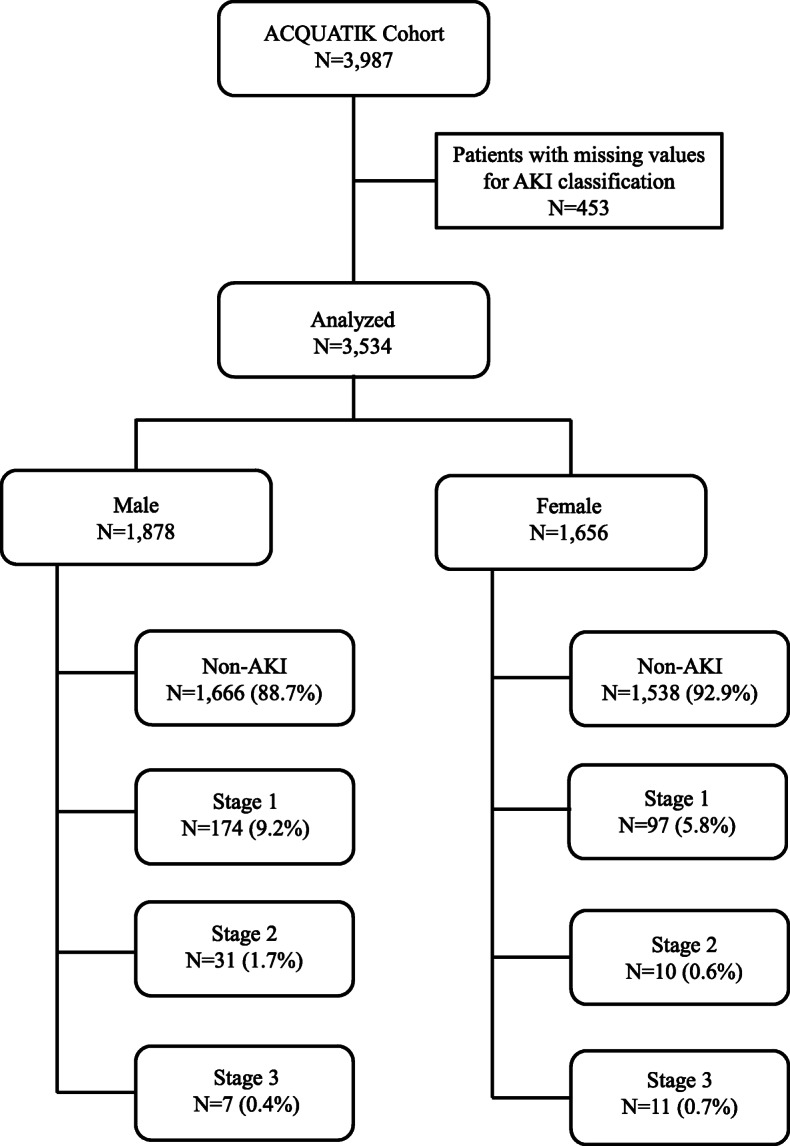
We included 3534 patients (1878 males with mean age 61.1 ± 17.7 and 1656 females 1656 with mean age 60.3 ± 20.0 years) admitted to Queen Elizabeth or Heartlands Hospitals, Birmingham, between October 2013 and January 2016. Patients were prospectively followed-up for a median 47.70 [IQR, 18.20] months. Study-endpoints were incidence of AKI, based on KDIGO-AKI Guidelines, and all-cause mortality. Data acquisition was automated, and information on mortality was collected from the Hospital Episode Statistics and Office of National Statistics. Socioeconomic status was evaluated with the Index of Multiple Deprivation (IMD).
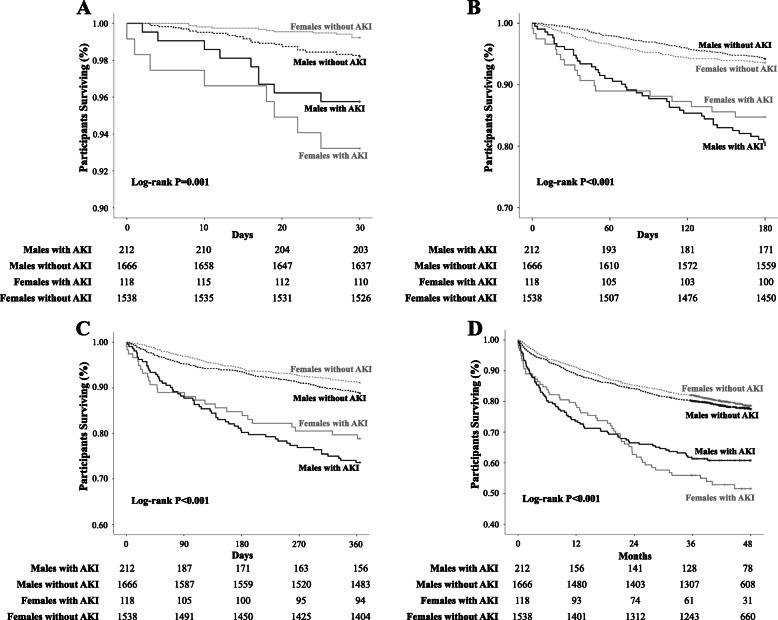
Incidence of AKI was higher in men compared to women (11.3% vs 7.1%; P < 0.001). Model regression analysis revealed significant association of male sex with higher AKI risk (OR, 1.659; 95% CI, 1.311-2.099; P < 0.001); this association remained significant after adjustment for age, eGFR, IMD, smoking, alcohol consumption, ethnicity, existing comorbidities and treatment (OR, 1.599; 95% CI, 1.215-2.103; P = 0.001). All-cause mortality was higher in patients with compared to those without AKI. Males with AKI had higher mortality rates in the first 6-month and 1-year periods after the index AKI event. The association of male sex with mortality was independent of socioeconomic factors but was not statistically significant after adjustment for existing comorbidities.
Men are at higher risk of AKI and this association is independent from existing risk factors for AKI. The association between male sex and AKI-related mortality was not independent from existing comorbidities. A better understanding of factors associated with AKI may help accurately identify high-risk patients.
多种合并症(包括糖尿病、高血压、心血管疾病、心力衰竭和慢性肾脏或肝脏疾病)与急性肾损伤(AKI)相关已得到充分证实。关于性别和社会经济因素的影响证据很少。本研究旨在探讨性别和社会经济因素与 AKI 及 AKI 相关死亡率的关系,并进一步评估与 AKI 发生的其他可能危险因素的额外关系。
我们纳入了 2013 年 10 月至 2016 年 1 月期间在伯明翰伊丽莎白女王医院或心胸医院住院的 3534 名患者(男性 1878 名,平均年龄 61.1±17.7 岁,女性 1656 名,平均年龄 60.3±20.0 岁)。前瞻性随访中位时间为 47.70[IQR,18.20]个月。研究终点为基于 KDIGO-AKI 指南的 AKI 发生率和全因死亡率。数据采集是自动化的,死亡率信息是从医院发病统计和国家统计局收集的。社会经济地位用多重剥夺指数(IMD)评估。
与女性相比,男性 AKI 的发生率更高(11.3%比 7.1%;P<0.001)。模型回归分析显示,男性与 AKI 风险增加显著相关(OR,1.659;95%CI,1.311-2.099;P<0.001);在调整年龄、eGFR、IMD、吸烟、饮酒、种族、并存疾病和治疗后,这种关联仍然显著(OR,1.599;95%CI,1.215-2.103;P=0.001)。与无 AKI 患者相比,AKI 患者的全因死亡率更高。发生 AKI 的男性在 AKI 事件发生后的前 6 个月和 1 年内死亡率更高。男性与死亡率之间的相关性独立于社会经济因素,但在调整并存疾病后无统计学意义。
男性发生 AKI 的风险更高,这种关联独立于 AKI 的现有危险因素。男性与 AKI 相关死亡率之间的关系不独立于现有的合并症。更好地了解与 AKI 相关的因素可能有助于准确识别高危患者。