Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, 553 St Kilda Road, Melbourne, VIC, 3004, Australia.
Department of Intensive Care and Hyperbaric Medicine, The Alfred, Melbourne, VIC, Australia.
Intensive Care Med. 2024 Sep;50(9):1470-1483. doi: 10.1007/s00134-024-07564-8. Epub 2024 Aug 20.
Patients receiving venoarterial extracorporeal membrane oxygenation (VA-ECMO) frequently develop arterial hyperoxaemia, which may be harmful. However, lower oxygen saturation targets may also lead to harmful episodes of hypoxaemia.
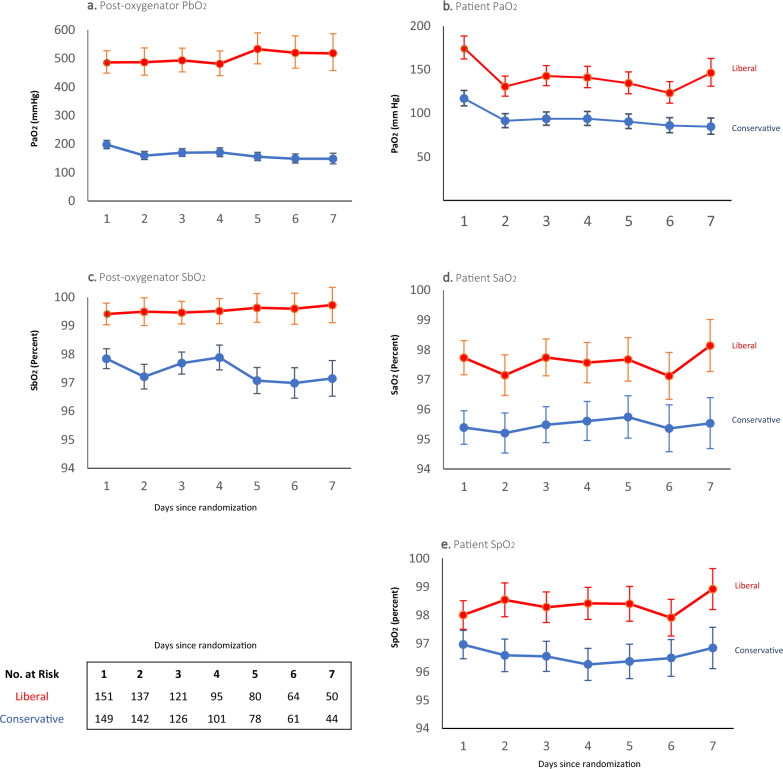
In this registry-embedded, multicentre trial, we randomly assigned adult patients receiving VA-ECMO in an intensive care unit (ICU) to either a conservative (target SaO 92-96%) or to a liberal oxygen strategy (target SaO 97-100%) through controlled oxygen administration via the ventilator and ECMO gas blender. The primary outcome was the number of ICU-free days to day 28. Secondary outcomes included ICU-free days to day 60, mortality, ECMO and ventilation duration, ICU and hospital lengths of stay, and functional outcomes at 6 months.
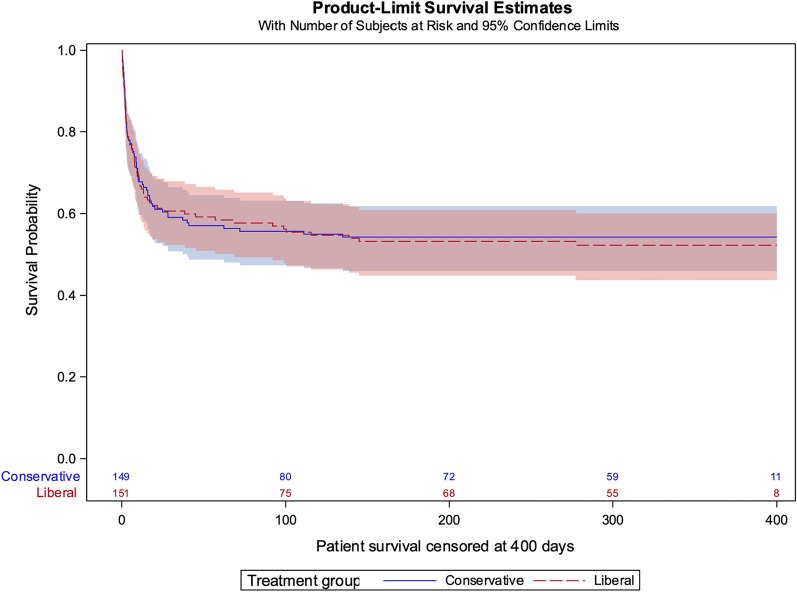
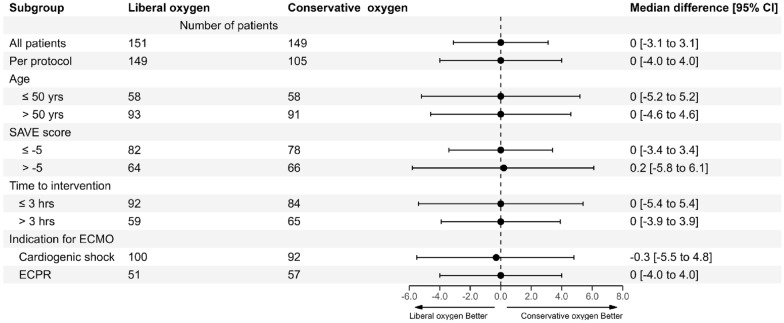
From September 2019 through June 2023, 934 patients who received VA-ECMO were reported to the EXCEL registry, of whom 300 (192 cardiogenic shock, 108 refractory cardiac arrest) were recruited. We randomised 149 to a conservative and 151 to a liberal oxygen strategy. The median number of ICU-free days to day 28 was similar in both groups (conservative: 0 days [interquartile range (IQR) 0-13.7] versus liberal: 0 days [IQR 0-13.7], median treatment effect: 0 days [95% confidence interval (CI) - 3.1 to 3.1]). Mortality at day 28 (59/159 [39.6%] vs 59/151 [39.1%]) and at day 60 (64/149 [43%] vs 62/151 [41.1%] were similar in conservative and liberal groups, as were all other secondary outcomes and adverse events. The conservative group experienced 44 (29.5%) major protocol deviations compared to 2 (1.3%) in the liberal oxygen group (P < 0.001).
In adults receiving VA-ECMO in ICU, a conservative compared to a liberal oxygen strategy, did not affect the number of ICU-free days to day 28.
接受体外膜肺氧合(VA-ECMO)治疗的患者常发生动脉高氧血症,这可能是有害的。然而,较低的氧饱和度目标也可能导致有害的低氧血症发作。
在这项注册嵌入式、多中心试验中,我们通过呼吸机和 ECMO 气体混合器对 ICU 中接受 VA-ECMO 治疗的成年患者进行随机分组,分别采用保守(目标 SaO2 92-96%)或宽松氧合策略(目标 SaO2 97-100%)。主要结局是至第 28 天无 ICU 天数。次要结局包括至第 60 天的 ICU 无天数、死亡率、ECMO 和通气持续时间、ICU 和住院时间以及 6 个月时的功能结局。
2019 年 9 月至 2023 年 6 月,EXCEL 登记处报告了 934 例接受 VA-ECMO 治疗的患者,其中 300 例(192 例心源性休克,108 例难治性心脏骤停)入选。我们将 149 例随机分配至保守氧合组,151 例随机分配至宽松氧合组。两组至第 28 天的 ICU 无天数中位数相似(保守组:0 天[四分位距(IQR)0-13.7];宽松组:0 天[IQR 0-13.7];中位治疗效果:0 天[95%置信区间(CI)-3.1 至 3.1])。第 28 天(59/159[39.6%]vs 59/151[39.1%])和第 60 天(64/149[43%]vs 62/151[41.1%])的死亡率在保守组和宽松组相似,其他次要结局和不良事件也相似。与宽松氧合组相比,保守氧合组发生 44 例(29.5%)主要方案偏离,而宽松氧合组仅发生 2 例(1.3%)(P<0.001)。
在 ICU 中接受 VA-ECMO 治疗的成年人中,与宽松氧合策略相比,保守氧合策略并未影响至第 28 天的无 ICU 天数。