Zhejiang University School of Medicine, Hangzhou, China (X.X., L.Z.).
Cardiovascular Imaging Program, Departments of Medicine and Radiology (X.X., S. Divakaran, B.N.W., J.H., S.S.L., B.A., M.F.K., R.B., S. Dorbala, J.M.B., M.F.D.C.), Brigham and Women's Hospital, Harvard Medical School, Boston, MA.
Circulation. 2024 Oct;150(14):1075-1086. doi: 10.1161/CIRCULATIONAHA.123.067083. Epub 2024 Aug 21.
Coronary microvascular dysfunction has been implicated in the development of hypertensive heart disease and heart failure, with subendocardial ischemia identified as a driver of sustained myocardial injury and fibrosis. We aimed to evaluate the relationships of subendocardial perfusion with cardiac injury, structure, and a composite of major adverse cardiac and cerebrovascular events consisting of death, heart failure hospitalization, myocardial infarction, and stroke.
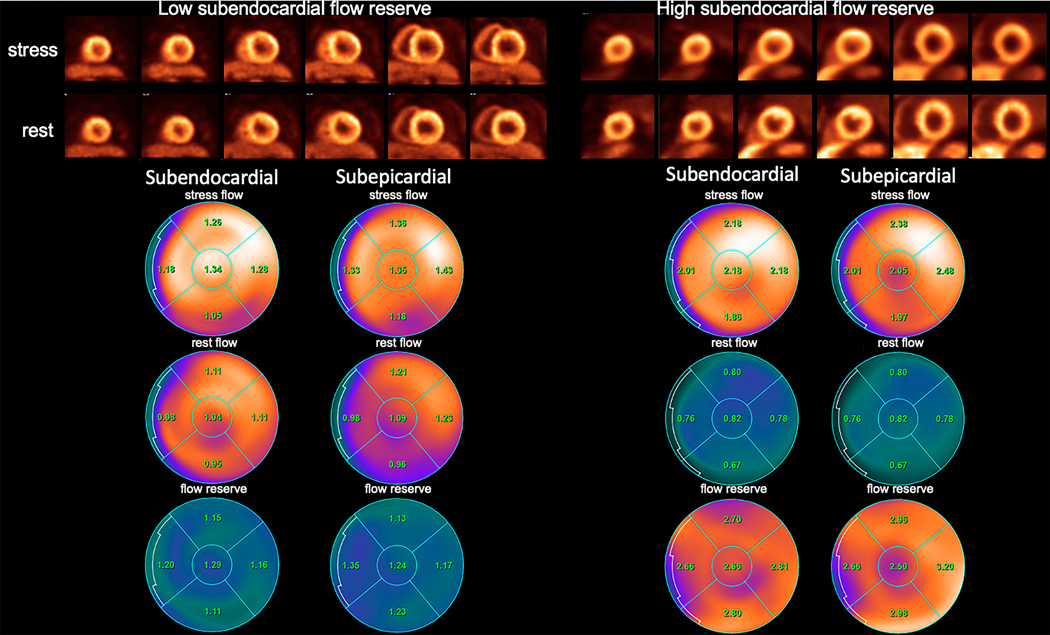
Layer-specific blood flow and myocardial flow reserve (MFR; stress/rest myocardial blood flow) were assessed by N-ammonia perfusion positron emission tomography in consecutive patients with hypertension without flow-limiting coronary artery disease (summed stress score <3) imaged at Brigham and Women's Hospital (Boston, MA) from 2015 to 2021. In this post hoc observational study, biomarkers, echocardiographic parameters, and longitudinal clinical outcomes were compared by tertiles of subendocardial MFR (MFR).
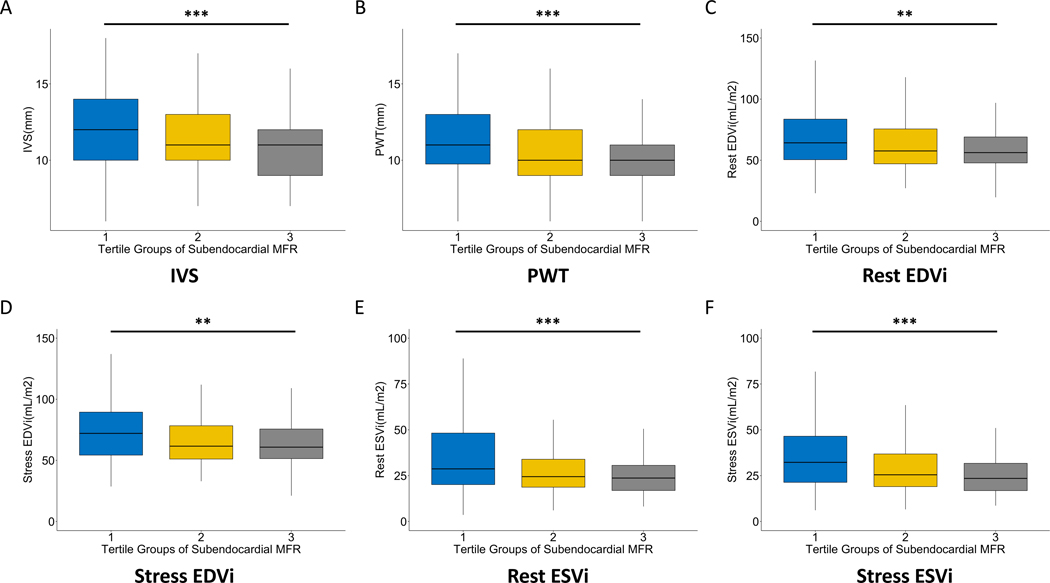
Among 358 patients, the mean age was 70.6±12.0 years, and 53.4% were male. The median MFR was 2.57 (interquartile range, 2.08-3.10), and lower MFR was associated with older age, diabetes, lower renal function, greater coronary calcium burden, and higher systolic blood pressure (<0.05 for all). In cross-sectional multivariable regression analyses, the lowest tertile of MFR was associated with myocardial injury and with greater left ventricular wall thickness and volumes compared with the highest tertile. Relative to the highest tertile, low MFR was independently associated with an increased rate of major adverse cardiac and cerebrovascular events (adjusted hazard ratio, 2.99 [95% CI, 1.39-6.44]; =0.005) and heart failure hospitalization (adjusted hazard ratio, 2.76 [95% CI, 1.04-7.32; =0.042) over 1.1 (interquartile range, 0.6-2.8) years median follow-up.
Among patients with hypertension without flow-limiting coronary artery disease, impaired MFR was associated with cardiovascular risk factors, elevated cardiac biomarkers, cardiac structure, and clinical events.
冠状动脉微血管功能障碍与高血压性心脏病和心力衰竭的发展有关,其中心内膜下缺血被认为是持续心肌损伤和纤维化的驱动因素。我们旨在评估心内膜下灌注与心脏损伤、结构以及由死亡、心力衰竭住院、心肌梗死和中风组成的主要不良心脏和脑血管事件的复合事件的关系。
2015 年至 2021 年,在布莱根妇女医院(波士顿,MA)连续成像的无限制冠状动脉疾病(总和应激评分<3)的高血压患者中,通过 N-氨灌注正电子发射断层扫描评估层特异性血流和心肌血流储备(应激/休息心肌血流)。在这项事后观察性研究中,根据心内膜下 MFR(MFR)的三分位数,比较生物标志物、超声心动图参数和纵向临床结局。
在 358 例患者中,平均年龄为 70.6±12.0 岁,53.4%为男性。中位 MFR 为 2.57(四分位距,2.08-3.10),较低的 MFR与年龄较大、糖尿病、较低的肾功能、更高的冠状动脉钙负荷和更高的收缩压有关(所有<0.05)。在横断面多变量回归分析中,MFR 的最低三分位数与心肌损伤以及与左心室壁厚度和体积较大相关。与最高三分位数相比,低 MFR 与主要不良心脏和脑血管事件(调整后的危险比,2.99[95%CI,1.39-6.44];=0.005)和心力衰竭住院(调整后的危险比,2.76[95%CI,1.04-7.32;=0.042)的发生率增加独立相关,中位随访 1.1(四分位距,0.6-2.8)年。
在无限制冠状动脉疾病的高血压患者中,MFR 受损与心血管危险因素、升高的心脏生物标志物、心脏结构和临床事件相关。