Department of Hematology, Tsukuba University Hospital Mito Clinical Education and Training Center, 3-2-7 Miya-Cho, Mito, Ibaraki, Japan.
Health Services Research and Development Center, University of Tsukuba, Ibaraki, Japan.
BMC Geriatr. 2024 Aug 21;24(1):696. doi: 10.1186/s12877-024-05296-4.
Older adults requiring care often have multiple morbidities that lead to polypharmacy, including the use of potentially inappropriate medications (PIMs), leading to increased medical costs and adverse drug effects. We conducted a cross-sectional study to clarify the actual state of drug prescriptions and the background of polypharmacy and PIMs.
Using long-term care (LTC) and medical insurance claims data in the Ibaraki Prefecture from April 2018 to March 2019, we included individuals aged ≥ 65 who used LTC services. The number of drugs prescribed for ≥ 14 days and the number of PIMs were counted. A generalized linear model was used to analyze the association between the backgrounds of individuals and the number of drugs; logistic regression analysis was used for the presence of PIMs. PIMs were defined by STOPP-J and Beers Criteria.
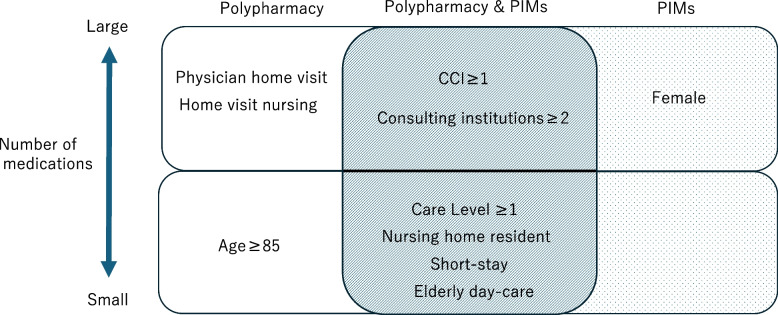
Herein, 67,531 older adults who received LTC services were included. The median number of total prescribed medications and PIMs was 7(IQR 5-9) and 1(IQR 0-1), respectively. The main PIMs were loop diuretics/aldosterone antagonists (STOPP-J), long-term use of proton pump inhibitors (Beers Criteria), benzodiazepines/similar hypnotics (STOPP-J and Beers Criteria), and nonsteroidal anti-inflammatory drugs (STOPP-J and Beers Criteria). Multivariate analysis revealed that the number of medications and presence of PIMs were significantly higher in patients with comorbidities and in those visiting multiple medical institutions. However, patients requiring care level ≥1, nursing home residents, users of short-stay service, and senior daycare were negatively associated with polypharmacy and PIMs.
Polypharmacy and PIMs are frequently observed in older adults who require LTC. This was prominent among individuals with comorbidities and at multiple consulting institutions. Utilization of nursing care facilities may contribute to reducing polypharmacy and PIMs.
需要护理的老年人通常患有多种疾病,导致多种药物治疗,包括使用潜在不适当的药物(PIMs),导致医疗费用增加和药物不良反应增加。我们进行了一项横断面研究,以阐明药物处方的实际状况以及多药治疗和 PIMs 的背景。
我们使用了 2018 年 4 月至 2019 年 3 月茨城县的长期护理(LTC)和医疗保险索赔数据,纳入了使用 LTC 服务的年龄≥65 岁的个体。计算了处方的药物数量(≥14 天)和 PIMs 的数量。使用广义线性模型分析个体背景与药物数量之间的关联;使用逻辑回归分析 PIMs 的存在。PIMs 通过 STOPP-J 和 Beers 标准定义。
本研究共纳入 67531 名接受 LTC 服务的老年人。总处方药物和 PIMs 的中位数分别为 7(IQR 5-9)和 1(IQR 0-1)。主要的 PIMs 是噻嗪类利尿剂/醛固酮拮抗剂(STOPP-J)、质子泵抑制剂的长期使用(Beers 标准)、苯二氮䓬类/类似催眠药(STOPP-J 和 Beers 标准)和非甾体抗炎药(STOPP-J 和 Beers 标准)。多变量分析显示,患有合并症的患者和就诊于多家医疗机构的患者的药物数量和 PIMs 的存在显著更高。然而,需要护理水平≥1、养老院居民、短期服务使用者和高级日托中心的使用者与多药治疗和 PIMs 呈负相关。
需要 LTC 的老年人中经常出现多药治疗和 PIMs。这在患有合并症和在多家医疗机构就诊的个体中更为突出。护理设施的使用可能有助于减少多药治疗和 PIMs。