Baumer-Mouradian Shannon H, Bradley Lia C, Ansari Sadia T, Chinta Sri S, Mitchell Michelle L, Nelson Anika M, Marusinec Laura E, Wake Kristine M, Mantey Karie A, Cabrera Ilanalee C, De Valk Jessica A, Hanson Aaron P, Witkowski Elizabeth M, Bushee Glenn M, Ellison Jonathan S
From the Department of Pediatrics, Medical College of Wisconsin, Children's Corporate Center, Milwaukee, Wis.
Quality Department, Children's Wisconsin, Wauwatosa, Wis.
Pediatr Qual Saf. 2024 Aug 21;9(5):e756. doi: 10.1097/pq9.0000000000000756. eCollection 2024 Sep-Oct.
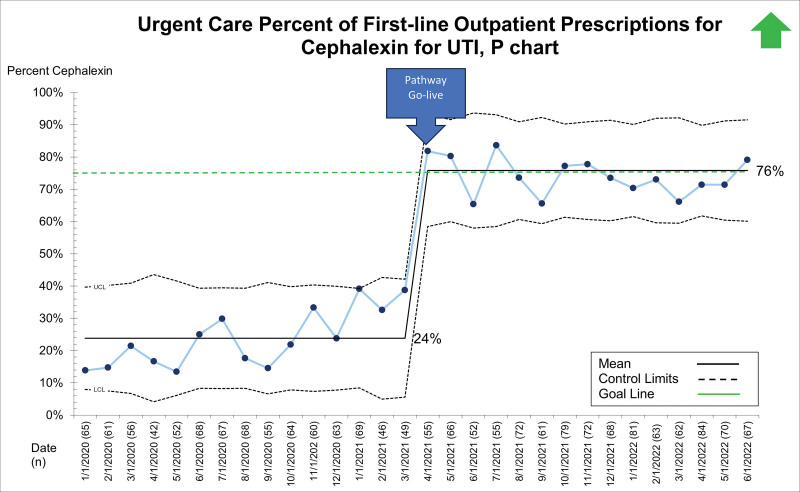
Pediatric urinary tract infections (UTIs) require early diagnosis and appropriate treatment to avoid short- and long-term morbidity. Baseline data from 13,000 children across a regional health system demonstrated wide variation in UTI management, including antibiotic choice, duration, and dosing. In 2019, the local antibiotic stewardship team recommended cephalexin as the ideal first-line UTI treatment due to its effectiveness, narrow spectrum, low cost, and palatability. This project aimed to improve first-line prescription of cephalexin as an empiric antibiotic treatment for uncomplicated UTIs from 34% to 75% in children 60 days to 18 years of age presenting to any site within the healthcare system within 6 months.
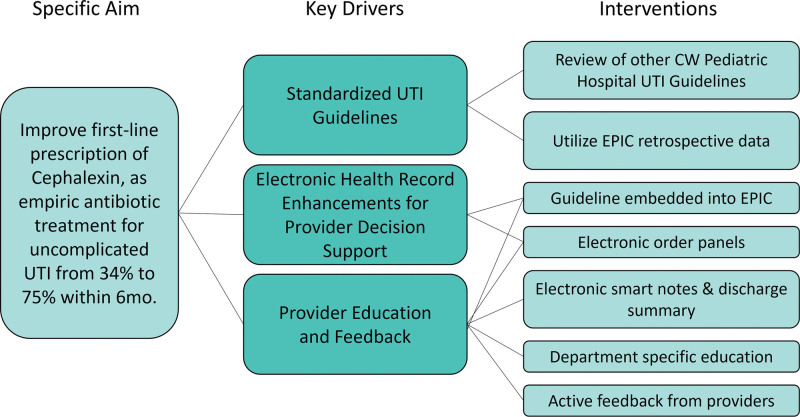
A multidisciplinary team of key stakeholders reviewed baseline data and developed three key drivers. These included a standardized UTI pathway, electronic health record enhancements, and provider education. Interventions were supported by a literature review and implemented via Plan-Do-Study-Act cycles with data monitored bimonthly. The primary outcome was the percentage of patients prescribed cephalexin for presumed UTI over the total number of presumed UTI diagnoses treated with empiric antibiotics throughout the healthcare system. The balancing measure included 14-day return visits for a UTI-related diagnosis across the system.
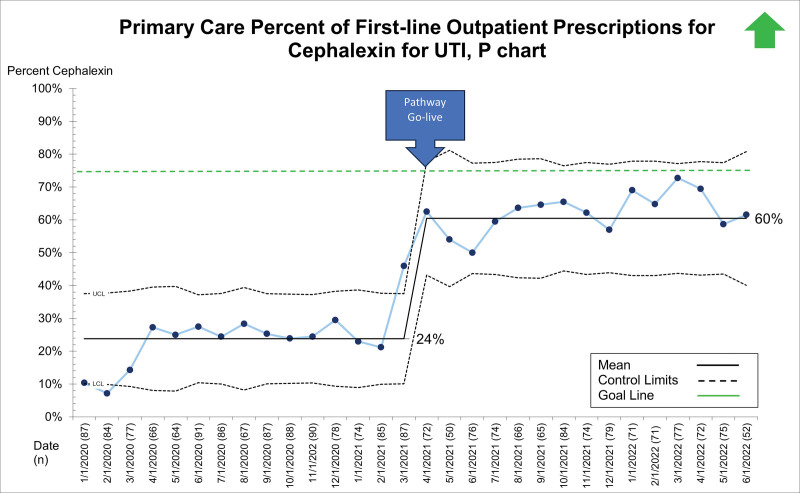
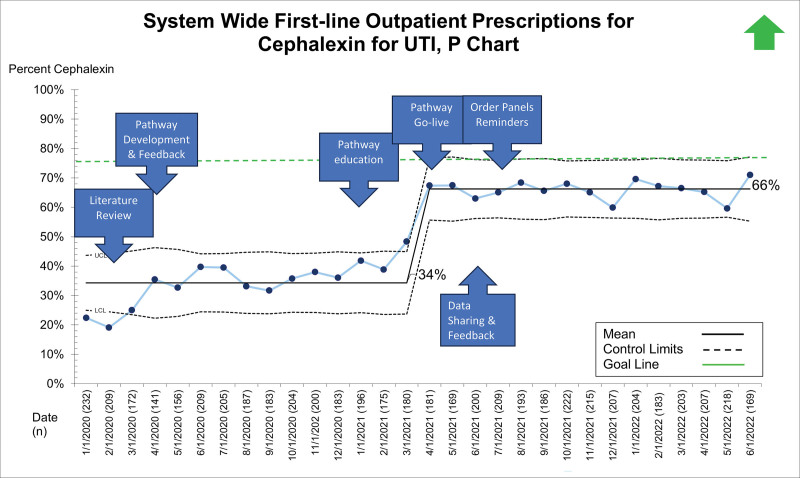
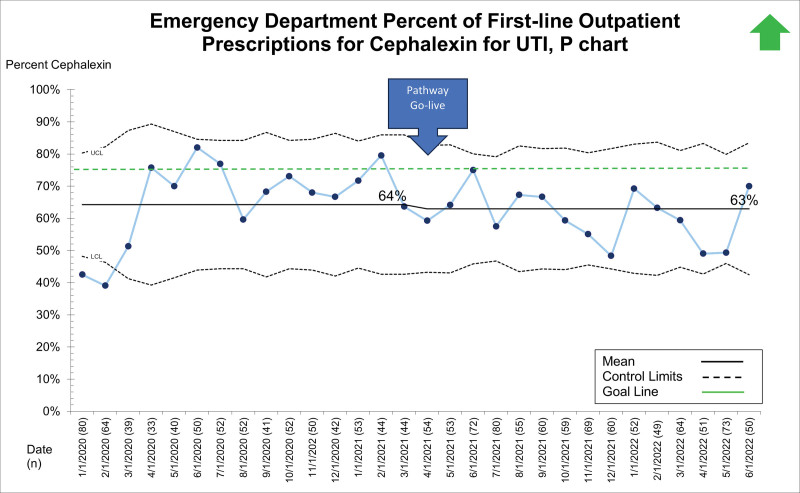
After the release of the updated UTI pathway, first-line cephalexin prescribing for UTI improved from 34% to 66%. There was no change in 14-day revisits for UTI.
Standardizing the diagnosis and management of UTIs across the spectrum of coordinated care led to improved system-wide adherence to local antibiotic stewardship guidelines for empiric UTI treatment.
儿童尿路感染(UTIs)需要早期诊断和适当治疗,以避免短期和长期发病。来自一个区域卫生系统的13000名儿童的基线数据显示,UTI管理存在很大差异,包括抗生素选择、疗程和剂量。2019年,当地抗生素管理团队推荐头孢氨苄作为理想的一线UTI治疗药物,因其有效性、窄谱、低成本和适口性。该项目旨在将头孢氨苄作为60天至18岁儿童单纯性UTI经验性抗生素治疗的一线处方率在6个月内从34%提高到75%,这些儿童在医疗系统内的任何地点就诊。
一个由关键利益相关者组成的多学科团队审查了基线数据,并确定了三个关键驱动因素。这些因素包括标准化的UTI诊疗路径、电子健康记录的改进以及提供者教育。干预措施得到文献综述的支持,并通过计划-执行-研究-改进循环实施,每两个月监测一次数据。主要结果是在整个医疗系统中,因疑似UTI而开具头孢氨苄处方的患者占接受经验性抗生素治疗的疑似UTI诊断总数的百分比。平衡指标包括整个系统中与UTI相关诊断的14天复诊率。
更新后的UTI诊疗路径发布后,UTI的一线头孢氨苄处方率从34%提高到了66%。UTI的14天复诊率没有变化。
在整个协调护理范围内对UTI的诊断和管理进行标准化,提高了全系统对UTI经验性治疗的当地抗生素管理指南的依从性。