Youngstrom Daniel W, Sutton Trevor S, Kabala Fleur S, Rosenzweig Isabella C, Johndro Charles W, Al-Araji Rabab, Burke-Martindale Carolyn, Mather Jeff F, McKay Raymond G
Hartford HealthCare Emergency Medical Services Network, 450 West Main Street, Meriden, CT 06451, USA.
Department of Anesthesiology, University of Connecticut School of Medicine, 263 Farmington Avenue, Farmington, CT 06030, USA.
Resusc Plus. 2024 Jul 27;19:100727. doi: 10.1016/j.resplu.2024.100727. eCollection 2024 Sep.
Prior reports have demonstrated underutilization of bystander cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) use in patients with witnessed out-of-hospital cardiac arrest (OHCA) in Connecticut. This study aimed to identify community-level risk factors that contribute to low rates of bystander intervention to improve statewide OHCA outcomes.
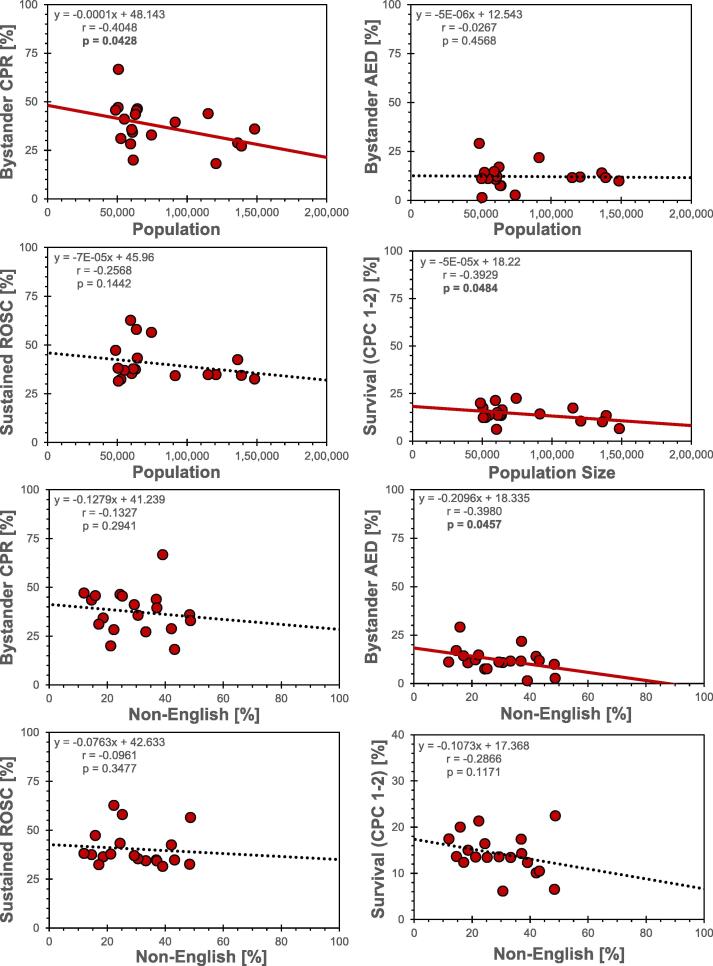
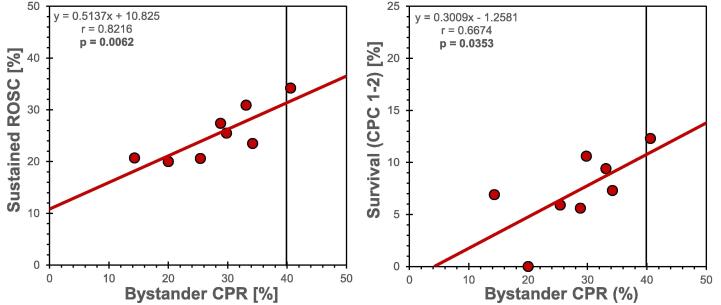
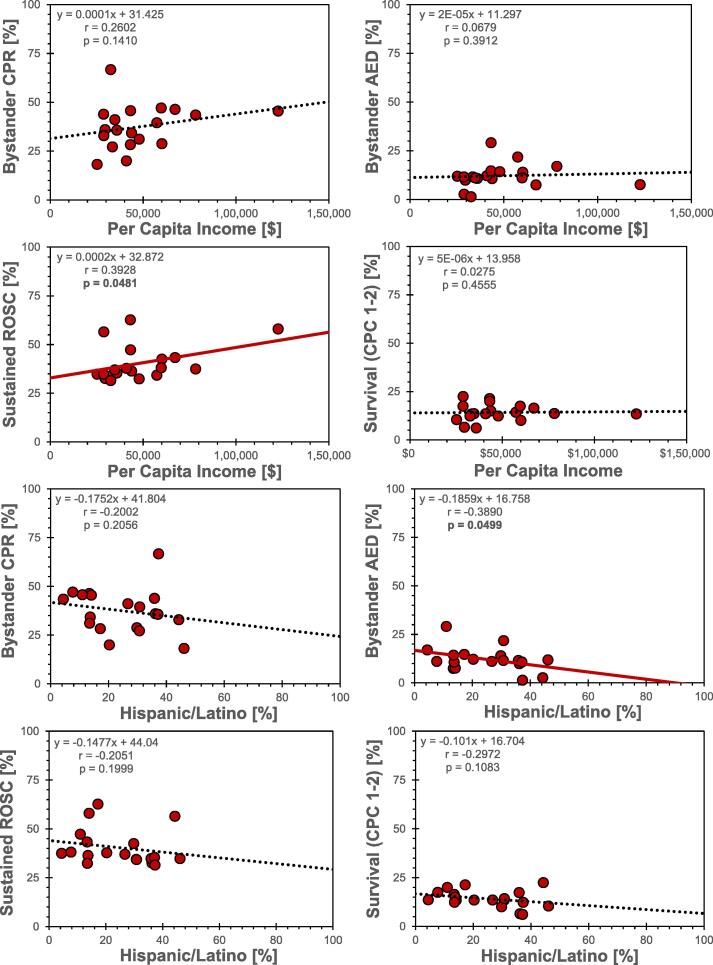
We analyzed 2,789 adult patients with witnessed, non-traumatic OHCA submitted to the Connecticut Cardiac Arrest Registry to Enhance Survival (CARES) between 2013-2022. Patients were grouped by zip code, and associated municipal characteristics were acquired from 2022 United States Census Bureau data. Use of bystander CPR, attempted bystander AED defibrillation, and patient survival with favorable neurological function were determined for 19 of the 20 most populous cities and towns. Pearson correlation tests and linear regression were used to determine associations between OHCA treatment and outcomes with population size, racial/ethnic demographics, language use, income, and educational level.
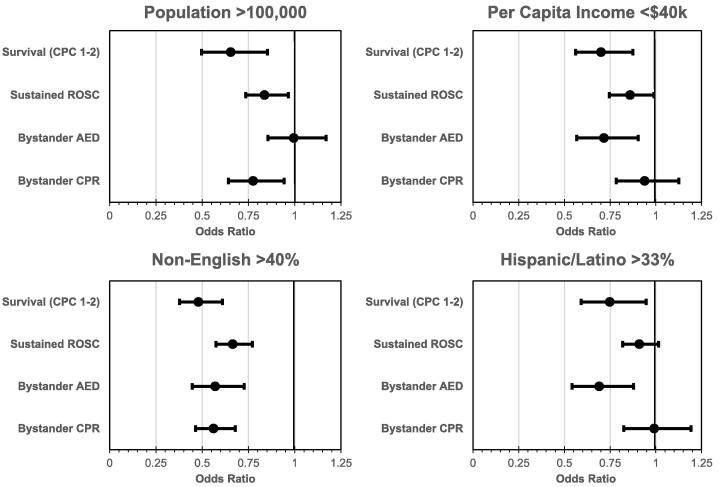
Bystander CPR was lower in municipalities with population size > 100,000 and in communities where > 40% of residents are non-English-speaking. AED use was also lower in these municipalities, as well as those with per capita incomes < $40,000 or > 1/3 Hispanic residents. Communities with populations > 100,000, > 40% non-English-speaking, per capita income < $40,000, and > 1/3 Hispanic residents were all associated with lower survival rates.
OHCA pre-hospital treatment and outcomes vary significantly by municipality in Connecticut. Community outcomes might be improved by specifically targeting urban population centers and Hispanic communities with culturally sensitive, low, or no-cost CPR and AED educational programs, using instructional languages other than English.
先前的报告表明,在康涅狄格州,院外心脏骤停(OHCA)患者中旁观者心肺复苏(CPR)和自动体外除颤器(AED)的使用未得到充分利用。本研究旨在确定导致旁观者干预率低的社区层面风险因素,以改善全州的OHCA结局。
我们分析了2013年至2022年间提交给康涅狄格州心脏骤停登记处以提高生存率(CARES)的2789例成年目击非创伤性OHCA患者。患者按邮政编码分组,并从2022年美国人口普查局数据中获取相关的市政特征。确定了20个人口最多的城镇中19个城镇的旁观者CPR使用情况、旁观者尝试进行AED除颤情况以及患者具有良好神经功能的生存率。使用Pearson相关检验和线性回归来确定OHCA治疗和结局与人口规模、种族/族裔人口统计、语言使用、收入和教育水平之间的关联。
在人口规模超过10万的市政当局以及居民中超过40%不讲英语的社区,旁观者CPR的使用率较低。这些市政当局以及人均收入低于4万美元或西班牙裔居民超过三分之一的市政当局中,AED的使用也较低。人口超过10万、不讲英语的居民超过40%、人均收入低于4万美元以及西班牙裔居民超过三分之一的社区,其生存率均较低。
在康涅狄格州,OHCA的院前治疗和结局因市政当局而异。通过以城市人口中心和西班牙裔社区为特定目标,使用英语以外的教学语言,开展具有文化敏感性、低成本或免费的CPR和AED教育项目,可能会改善社区结局。