Zimmerer Alexander, Nonnemacher Lars, Fischer Maximilian, Gebhardt Sebastian, Hofer André, Reichert Johannes, Wassilew Georgi
Klinik und Poliklinik für Orthopädie und Orthopädische Chirurgie, Universitätsmedizin Greifswald, Ferdinand-Sauerbruch-Str., 17475, Greifswald, Deutschland.
Orthopädische Klinik Paulinenhilfe, Stuttgart, Deutschland.
Oper Orthop Traumatol. 2024 Oct;36(5):280-291. doi: 10.1007/s00064-024-00860-y. Epub 2024 Aug 22.
Transfer of the gluteus maximus with refixation at the greater trochanter for treatment of abductor deficiency.
Symptomatic abductor deficiency with atrophy and fatty degeneration of the gluteal muscles > 50% (grade 3 by quartile) with good strength of the gluteus maximus.
Low atrophy or fatty degeneration of less than 50% of the gluteal muscles, limited strength of the gluteus maximus, infection.
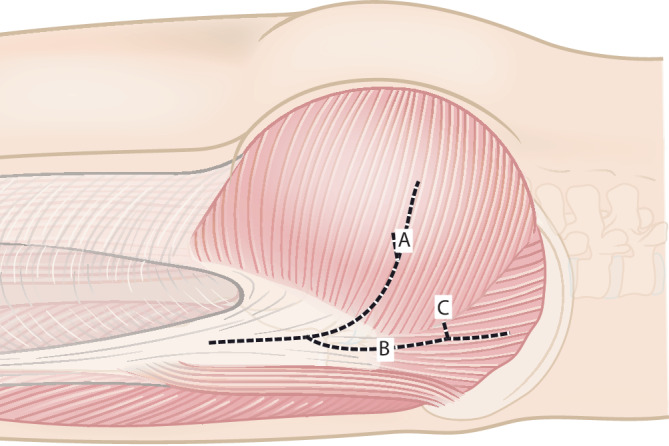
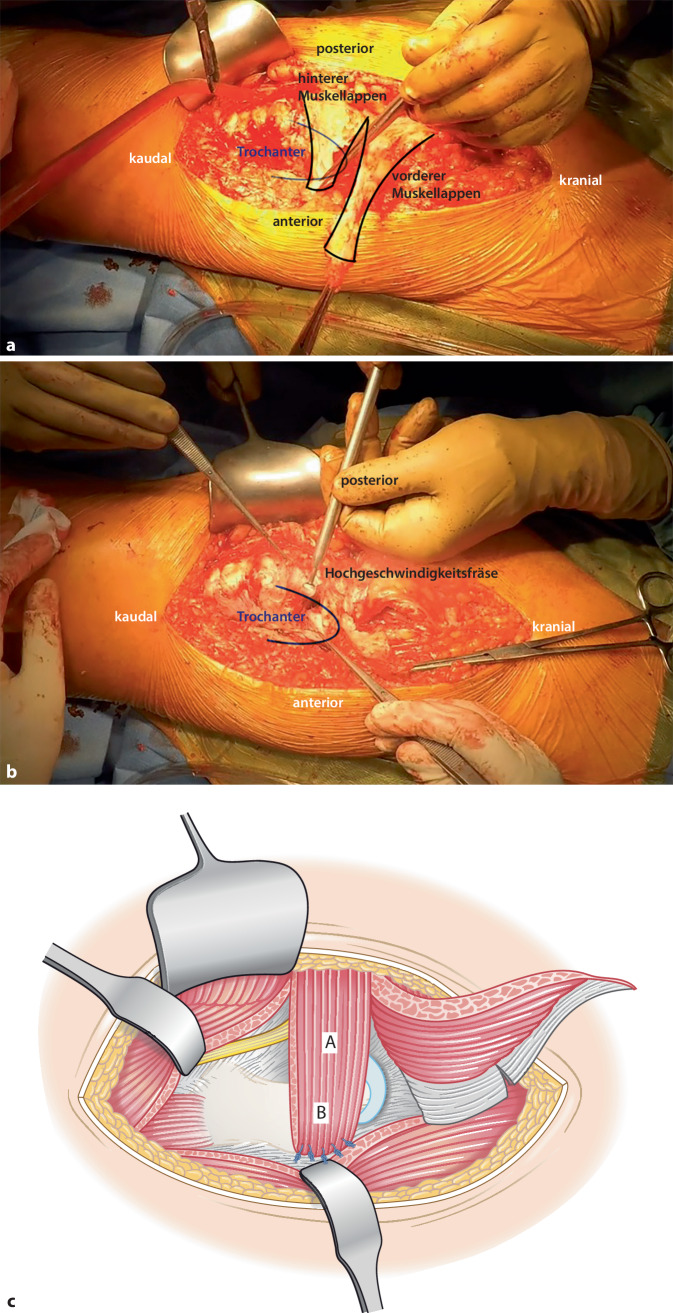
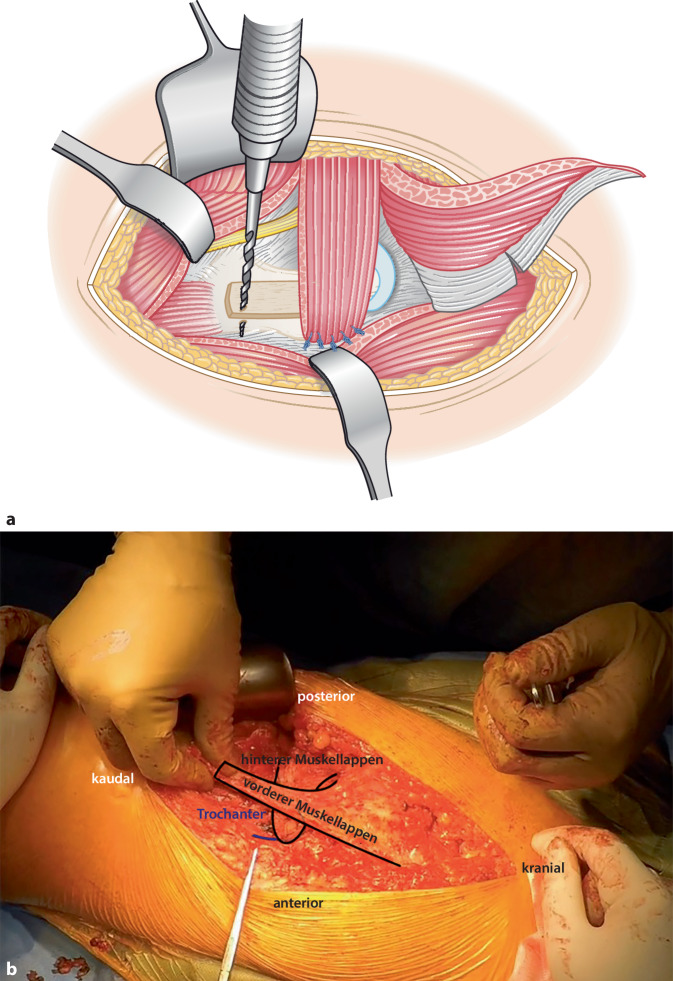
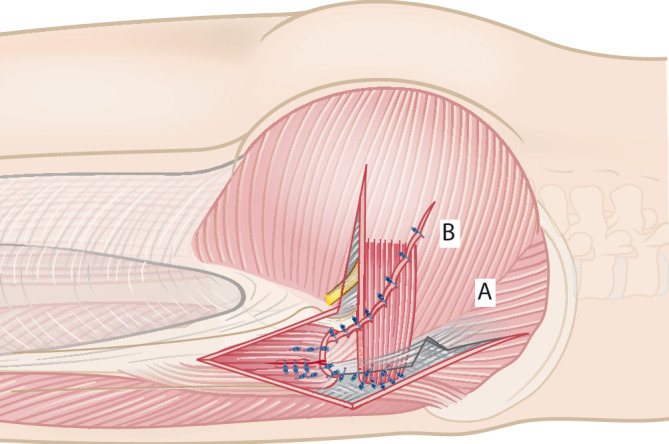
First, the fascia lata is incised dorsally to the tensor fascia latae muscle, with the incision extending approximately 1.5 cm proximal to the iliac crest. A second incision divides the gluteus maximus muscle longitudinally along the muscle fibers and continues towards the fascia lata distal to the greater trochanter. These incisions result in a triangular muscle flap, which is elevated and divided into anterior and posterior portions. The posterior flap is positioned ventrally over the femoral neck and fixed to the anterior capsule and the anterior edge of the greater trochanter. The anterior flap is placed directly on the proximal femur. For this purpose, a groove is prepared in the area of the proximal femur using a spherical burr to freshen up the future footprint. The anterior flap is positioned from the tip of the greater trochanter towards the insertion of the vastus lateralis muscle. Subsequently, the anterior flap is fixed to the created groove with transosseous sutures and positioned under the elevated vastus lateralis muscle in 15° abduction of the leg. To provide additional stabilization to the tendinous part of the anterior flap, a screw is inserted distally to the greater trochanter. The vastus lateralis muscle is attached to the distal tip of the anterior flap, and the remaining gluteus maximus muscle is sutured to the fascia lata to cover the anterior flap. Additionally, a flap of the tensor fascia latae muscle can be mobilized and adapted to the reconstruction. Layered wound closure is performed.
The technique of a gluteus maximus transfer represents a method for the treatment of chronic abductor deficiencies and improves abduction function as well as the gait pattern in short-term follow-ups. Fifteen patients (mean age at time of surgery 62 years) had after a mean follow-up of 2.5 years. The modified Harris Hip Score (mHHS) improved from 48 points preoperatively to 60 points at follow-up. Preoperatively, 100% had a positive Trendelenburg sign; at follow-up, this was about 50%.
通过在大转子处重新固定臀大肌来治疗外展肌功能不全。
有症状的外展肌功能不全,伴有臀肌萎缩和脂肪变性>50%(四分位数分级为3级),且臀大肌力量良好。
臀肌萎缩或脂肪变性低于50%,臀大肌力量受限,感染。
首先,在阔筋膜张肌背侧切开阔筋膜,切口在髂嵴近端约1.5厘米处延伸。第二个切口沿肌纤维纵向切开臀大肌,并向大转子远端的阔筋膜延伸。这些切口形成一个三角形肌瓣,将其掀起并分为前后两部分。后瓣置于股骨颈前方,固定于前关节囊和大转子前缘。前瓣直接置于股骨近端。为此,使用球形磨钻在股骨近端区域制备一个凹槽,以清理未来的附着点。前瓣从大转子尖端向股外侧肌止点方向放置。随后,用穿骨缝线将前瓣固定于制备好的凹槽,并在小腿外展15°时置于掀起的股外侧肌下方。为了给前瓣的腱性部分提供额外的稳定性,在大转子远端插入一枚螺钉。股外侧肌附着于前瓣远端尖端,剩余的臀大肌缝合于阔筋膜以覆盖前瓣。此外,可将阔筋膜张肌的一个肌瓣游离并用于重建。进行分层伤口缝合。
臀大肌转移技术是一种治疗慢性外展肌功能不全的方法,在短期随访中可改善外展功能和步态模式。15例患者(手术时平均年龄62岁)平均随访2.5年。改良Harris髋关节评分(mHHS)从术前的48分提高到随访时的60分。术前100%有阳性Trendelenburg征;随访时,这一比例约为50%。