University of Nebraska Medical Center, Omaha, NE, USA; James J. Peters Bronx Veterans Affairs Medical Center, Bronx, NY, USA.
Columbia University Herbert Irving Comprehensive Cancer Center, New York, NY, USA.
EBioMedicine. 2024 Sep;107:105288. doi: 10.1016/j.ebiom.2024.105288. Epub 2024 Aug 23.
We aimed to assess real-world efficacy of the PARP inhibitor, olaparib, in US Veterans with metastatic prostate cancer (mPC) by leveraging the national data repository and evaluate a novel approach to assess treatment efficacy in tumors considered rare or harboring rare mutations.
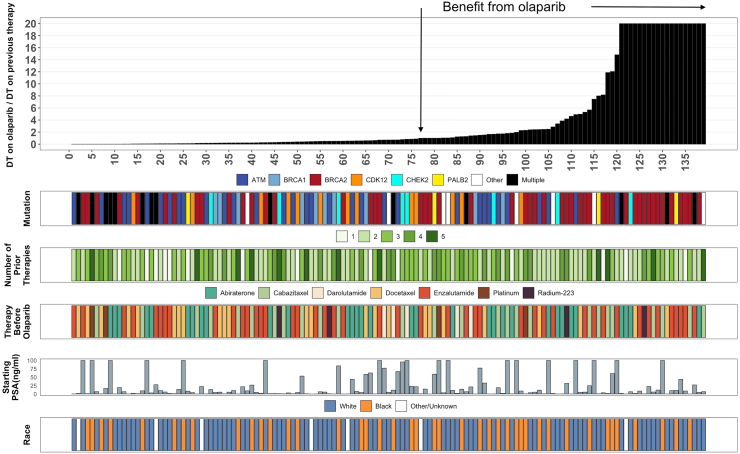
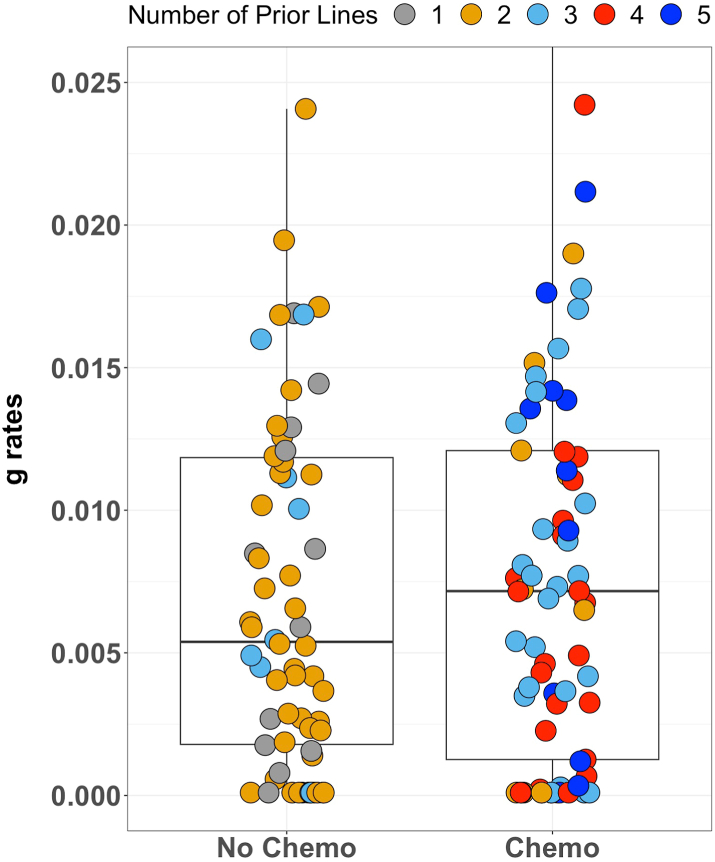
Included Veterans had 1) mPC with somatic or germline alterations/mutations in genes involved in homologous recombination repair (HRR), 2) received olaparib monotherapy as well as a novel hormonal therapy/androgen receptor pathway inhibitors (NHT/ARPI), and/or chemotherapy, and 3) estimable rates of tumor growth (g-rate) using PSA values obtained while receiving treatment. Previous work has shown an excellent inverse correlation of g-rate with survival. Using g-rate, we determined tumor doubling time (DT) and DT ratios (DT on olaparib/DT on prior medication). We postulated that a DT ratio≥ 1 was associated with benefit.
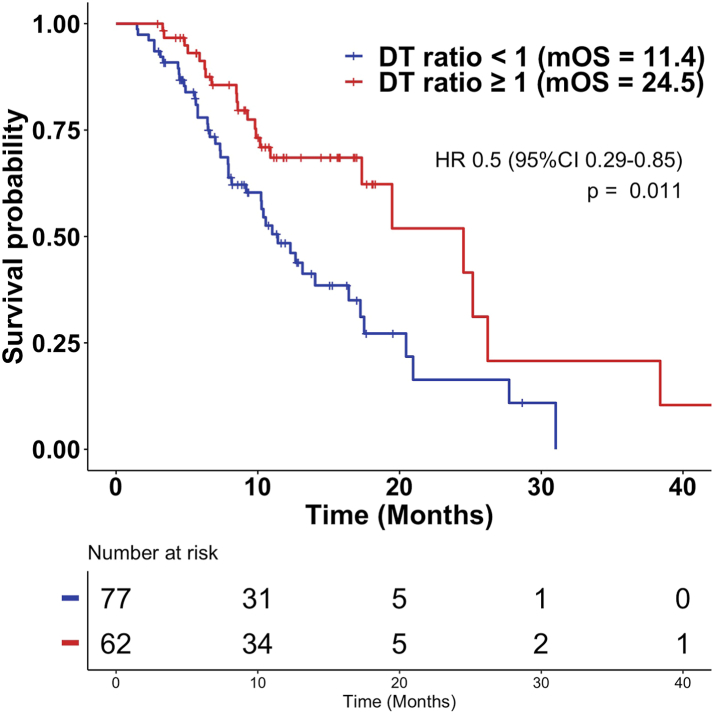
We identified 139 Veterans, including 42 Black males with tumors harboring mutations/alterations in HRR genes who received olaparib: BRCA2 (50), ATM (32), BRCA1 (10), other mutations (47). 62/139 (45%) of all and 21/42 (50%) of Black Veterans had DT ratios ≥1, including 31, 10, 2, and 19 with BRCA2, ATM, BRCA1, and other mutations, respectively (p = 0.006). Median survival with DT ratios ≥1 was superior, being 24.5 vs. 11.4 months for DT ratio <1 (p = 0.01, HR 0.50, 95% CI 0.29-0.85). Benefit from olaparib, defined as DT ratio ≥1, was not observed for germline status, starting PSA value, number of prior therapies, or immediate prior therapy. Compared to matched cohorts, tumors in the olaparib cohort had shorter DTs with enzalutamide in first line (367 vs. 884 days; p = 0.0043).
Using equations indifferent to timing of assessments ideal for real-world efficacy analyses, we showed DT ratio ≥1 representing slower tumor growth on olaparib relative to the prior therapy correlates with improved survival. Olaparib efficacy in Veterans with mPC harboring mutations/alterations in HRR genes emulates clinical trial results. Black men had comparable results. Compared to matched cohorts, in first line, enzalutamide was less efficacious in tumors harboring mutations/alterations in HRR genes.
American Society of Clinical Oncology Conquer Cancer Foundation (ASCO CCF), the Blavatnik Family Foundation and the Prostate Cancer Foundation (PCF).
我们旨在利用国家数据存储库评估 PARP 抑制剂奥拉帕利在有转移性前列腺癌(mPC)的美国退伍军人中的真实疗效,并评估一种评估被认为罕见或携带罕见突变的肿瘤治疗效果的新方法。
纳入的退伍军人符合以下条件:1)mPC 伴有同源重组修复(HRR)相关基因的体细胞或种系改变/突变;2)接受奥拉帕利单药治疗以及新的激素治疗/雄激素受体通路抑制剂(NHT/ARPI)和/或化疗;3)使用治疗期间获得的 PSA 值可估计肿瘤生长率(g-rate)。之前的工作表明 g-rate 与生存呈极好的负相关。使用 g-rate,我们确定了肿瘤倍增时间(DT)和 DT 比值(奥拉帕利治疗时的 DT/先前药物治疗时的 DT)。我们假设 DT 比值≥1 与获益相关。
我们确定了 139 名退伍军人,包括 42 名携带 HRR 基因突变/改变的黑人男性,他们接受了奥拉帕利治疗:BRCA2(50)、ATM(32)、BRCA1(10)、其他突变(47)。所有退伍军人的 62/139(45%)和黑人退伍军人的 21/42(50%)的 DT 比值≥1,分别包括 BRCA2、ATM、BRCA1 和其他突变的 31、10、2 和 19 名患者(p=0.006)。具有 DT 比值≥1 的中位生存时间更长,DT 比值<1 的中位生存时间为 24.5 个月,DT 比值≥1 的中位生存时间为 11.4 个月(p=0.01,HR 0.50,95%CI 0.29-0.85)。对于种系状态、起始 PSA 值、先前治疗次数或最近的治疗,未观察到定义为 DT 比值≥1 的奥拉帕利获益。与匹配队列相比,奥拉帕利队列中一线使用恩扎卢胺的肿瘤具有更短的 DT(367 天 vs. 884 天;p=0.0043)。
使用不依赖于评估时间的方程,对于真实世界疗效分析是理想的,我们表明,奥拉帕利治疗时 DT 比值≥1 代表肿瘤生长速度较慢,与生存改善相关。奥拉帕利在携带 HRR 基因突变/改变的 mPC 退伍军人中的疗效与临床试验结果一致。黑人男性的结果相似。与匹配队列相比,一线使用恩扎卢胺在携带 HRR 基因突变/改变的肿瘤中的疗效较差。
美国临床肿瘤学会征服癌症基金会(ASCO CCF)、布拉瓦特尼克家族基金会和前列腺癌基金会(PCF)。