Department of Medical and Surgical Sciences (DIMEC), Alma Mater Studiorum - University of Bologna, Via Massarenti, 9, 40138, Bologna, Italy.
Anesthesiology and General Intensive Care Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Crit Care. 2024 Aug 27;28(1):278. doi: 10.1186/s13054-024-05074-z.
Age as an eligibility criterion for V-V ECMO is widely debated and varies among healthcare institutions. We examined how age relates to mortality in patients undergoing V-V ECMO for ARDS.
Systematic review and meta-regression of clinical studies published between 2015 and June 2024. Studies involving at least 6 ARDS patients treated with V-V ECMO, with specific data on ICU and/or hospital mortality and patient age were included. The search strategy was executed in PubMed, limited to English-language. COVID-19 and non-COVID-19 populations were analyzed separately. Meta-regressions of mortality outcomes on age were performed using gender, BMI, SAPS II, APACHE II, Charlson comorbidity index or SOFA as covariates.
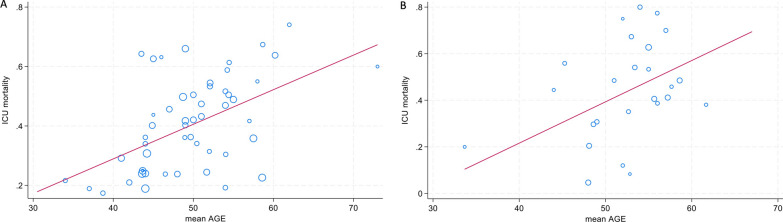
In non-COVID ARDS, the meta-regression of 173 studies with 56,257 participants showed a significant positive association between mean age and ICU/hospital mortality. In COVID-19 ARDS, a significant relationship between mean age and ICU mortality, but not hospital mortality, was found in 103 studies with 21,255 participants. Sensitivity analyses confirmed these findings, highlighting a linear relationship between age and mortality in both groups. For each additional year of mean age, ICU mortality increased by 1.2% in non-COVID ARDS and 1.9% in COVID ARDS.
The relationship between age and ICU mortality is linear and shows no inflection point. Consequently, no age cut-off can be recommended for determining patient eligibility for V-V ECMO.
年龄作为体外膜肺氧合(V-V ECMO)的入选标准存在广泛争议,且在不同医疗机构之间存在差异。我们研究了年龄与急性呼吸窘迫综合征(ARDS)患者接受 V-V ECMO 治疗后的死亡率之间的关系。
对 2015 年至 2024 年 6 月期间发表的临床研究进行系统回顾和荟萃回归分析。纳入了至少有 6 例 ARDS 患者接受 V-V ECMO 治疗、有 ICU 和/或医院死亡率及患者年龄具体数据的研究。检索策略在 PubMed 中执行,仅限于英文文献。分别分析 COVID-19 和非 COVID-19 人群。使用性别、BMI、简化急性生理学评分(SAPS)Ⅱ、急性生理与慢性健康评分系统Ⅱ(APACHE Ⅱ)、Charlson 合并症指数或序贯器官衰竭评估(SOFA)作为协变量,对死亡率与年龄的荟萃回归进行分析。
在非 COVID-19 ARDS 中,对 173 项研究(涉及 56257 例患者)的荟萃回归分析显示,平均年龄与 ICU/医院死亡率之间存在显著的正相关关系。在 COVID-19 ARDS 中,对 103 项研究(涉及 21255 例患者)的荟萃回归分析显示,平均年龄与 ICU 死亡率之间存在显著关系,但与医院死亡率无关。敏感性分析证实了这些发现,突出了两组中年龄与死亡率之间的线性关系。在非 COVID-19 ARDS 中,平均年龄每增加 1 岁,ICU 死亡率增加 1.2%;在 COVID-19 ARDS 中,ICU 死亡率增加 1.9%。
年龄与 ICU 死亡率之间的关系是线性的,且没有拐点。因此,不能推荐任何年龄截止值来确定患者接受 V-V ECMO 的资格。