Dohmen J, Weissinger D, Peter A S T, Theodorou A, Kalff J C, Stoffels B, Lingohr P, von Websky M
Department of Surgery, University of Bonn, Bonn, Germany.
Department of Surgery, Ippokrateio University Hospital Athens, Athens, Greece.
Front Surg. 2024 Aug 13;11:1449702. doi: 10.3389/fsurg.2024.1449702. eCollection 2024.
In emergency surgery, managing abdominal sepsis and critically ill patients with imminent abdominal compartment syndrome (ACS) using an open abdomen (OA) approach has become standard practice for damage control. To prevent significant complications associated with OA therapy, such as abdominal infections, entero-atmospheric fistula (EAF), and abdominal wall hernia formation, early definitive fascial closure (DFC) is crucial. This study aims to assess the feasibility of a novel device designed to facilitate early fascial closure in patients with an open abdomen.
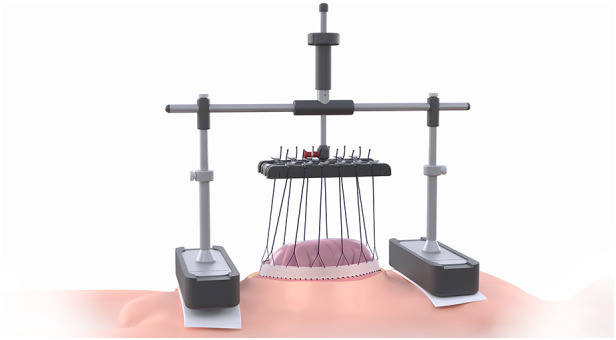
Between 2019 and 2020, nine patients undergoing open abdomen management were enrolled in this study. All patients were treated using vertical mesh-mediated fascial traction combined with a novel vertical traction device (VTD). Data from these cases were collected and retrospectively analyzed.
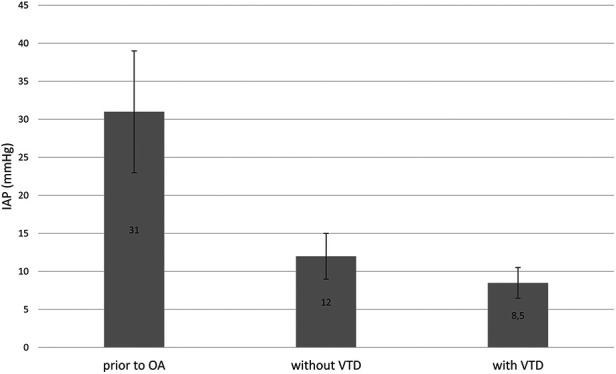
In this study, all patients were treated with OA due to impending ACS. Three patients died before achieving DFC, while the remaining six patients successfully underwent DFC. The mean number of surgical procedures after OA was 3 ± 1, and the mean time to DFC was 9 ± 3 days. The use of the VTD in combination with negative pressure wound therapy (NPWT) resulted in a 76% reduction in fascia-to-fascia distance until DFC was achieved. The application of the VTD did not affect ventilation parameters or the Simplified Acute Physiology Score II (SAPS II), but intra-abdominal pressure (IAP) was reduced from 31 ± 8 mmHg prior to OA to 8.5 ± 2 mmHg after applying the device. The primary complication associated with the device was skin irritation, with three patients developing skin blisters as the most severe manifestation.
Overall, the novel VTD appears to be a safe and feasible option for managing OA cases. It may reduce complications associated with OA by promoting early definitive fascial closure.
在急诊手术中,采用开放腹腔(OA)方法处理腹部脓毒症和即将发生腹腔间隔室综合征(ACS)的危重症患者已成为损伤控制的标准做法。为预防与OA治疗相关的严重并发症,如腹部感染、肠-气瘘(EAF)和腹壁疝形成,早期确定性筋膜关闭(DFC)至关重要。本研究旨在评估一种旨在促进开放腹腔患者早期筋膜关闭的新型装置的可行性。
2019年至2020年期间,9例接受开放腹腔处理的患者纳入本研究。所有患者均采用垂直网片介导的筋膜牵引联合新型垂直牵引装置(VTD)进行治疗。收集这些病例的数据并进行回顾性分析。
本研究中,所有患者均因即将发生的ACS接受OA治疗。3例患者在实现DFC前死亡,其余6例患者成功接受DFC。OA后的平均手术次数为3±1次,DFC的平均时间为9±3天。VTD与负压伤口治疗(NPWT)联合使用使至实现DFC时筋膜间距离减少了76%。VTD的应用未影响通气参数或简化急性生理学评分II(SAPS II),但腹腔内压力(IAP)从OA前的31±8 mmHg降至应用该装置后的8.5±2 mmHg。与该装置相关的主要并发症是皮肤刺激,3例患者出现皮肤水泡为最严重表现。
总体而言,新型VTD似乎是处理OA病例的一种安全可行的选择。它可能通过促进早期确定性筋膜关闭来减少与OA相关的并发症。