Department of Geriatrics, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse, 3010 Bern, Switzerland.
Department of Reconstructive Dentistry and Gerodontology, School of Dental Medicine, University of Bern, 3010 Bern, Switzerland.
Int J Environ Res Public Health. 2024 Jul 29;21(8):995. doi: 10.3390/ijerph21080995.
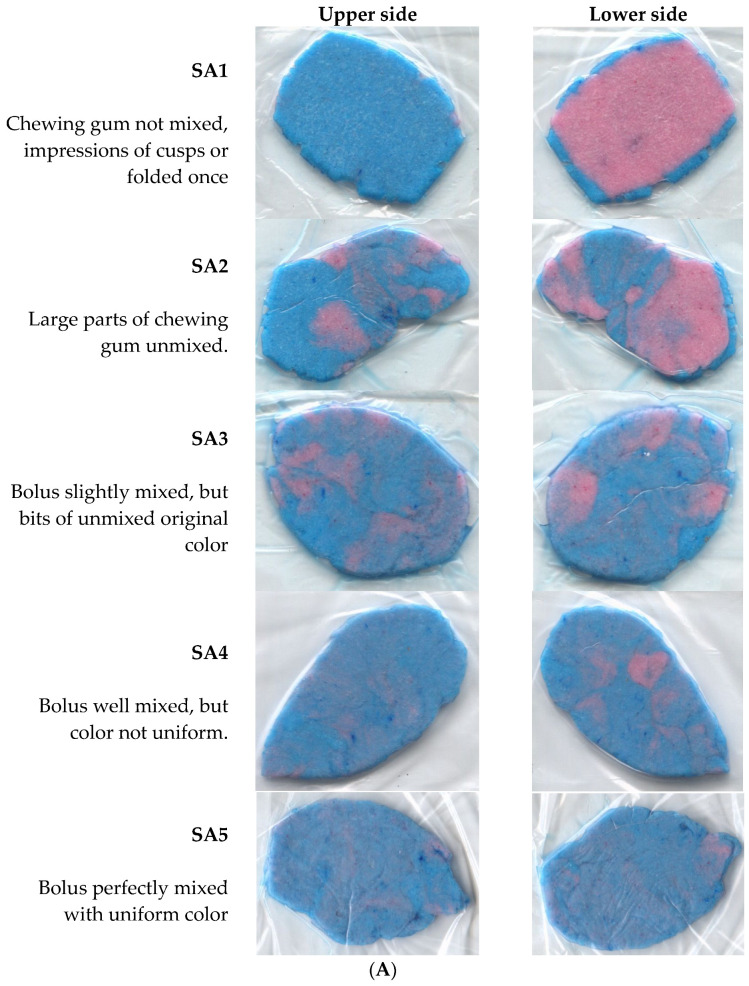
(1) Background: Insufficient data exist regarding oral function among older adults in Europe. Therefore, we aimed to assess and compare oral function between older in- and outpatients and identify predictors of low masticatory performance. (2) Methods: Patients were consecutively recruited from the outpatient center ( = 31) and the inpatient geriatric department ( = 31) at a tertiary University Hospital in Switzerland in 2023. Assessments on oral function included the total number of intraoral eruptive teeth, number of supporting zones with dentures, maximal bite force (Dental Prescale II, Fuji Film Corp., Tokyo, Japan), and masticatory performance (Hue-Check Gum©, University of Bern, Bern, Switzerland) using a visual (SA1-SA5) and a digital (SD_Hue) scale. The visual and digital assessment of masticatory performance showed a strong correlation (Kendall tau = 0.83). Low masticatory performance was defined as SA-Grade 1-2 (vs. SA3-SA5 as reference). In a multivariate model adjusting for age, sex, and clinical setting, we investigated associations of maximal bite force, few eruptive teeth, and few supporting zones with low masticatory performance. (3) Results: Mean age was 81.9 (standard deviation (sd) 5.2) years, and 62.9% were female. Overall, maximal bite force was 247 N (sd 261). A total of 39 patients (63.9%) had a low masticatory performance, 62.9% a low maximal bite force, and 50% a low number of eruptive teeth (<10). Masticatory performance, number of eruptive teeth, and maximal bite force did not significantly differ between in- and outpatients. The number of supporting zones was significantly higher in outpatients compared to inpatients (median 4, interquartile range (IQR) 4-4; vs. 4, IQR 2-4; = 0.03). In the multivariate model, maximal bite force and a low number of eruptive teeth were independently associated with low masticatory performance (adjusted odds ratio 7.4 (95% CI, 1.8-30.4; < 0.01), and OR 7.8 (95% CI, 1.7-36.4; < 0.01), respectively). (4) Conclusions: Impaired oral function is highly prevalent in both European older in- and outpatients to a similar degree. The association of low masticatory performance with maximal bite force and with a low number of eruptive teeth may indicate that a basic screening should include either of these parameters to identify impaired oral function.
(1) 背景:欧洲老年人的口腔功能相关数据不足。因此,我们旨在评估和比较老年住院和门诊患者的口腔功能,并确定咀嚼能力低的预测因素。(2) 方法:2023 年,我们在瑞士一所三级大学医院的门诊中心( = 31 例)和老年病房( = 31 例)连续招募患者。口腔功能评估包括口腔内萌出牙齿总数、有义齿支持区的数量、最大咬合力(Dental Prescale II,富士胶片公司,东京,日本)和咀嚼性能(Hue-Check Gum©,伯尔尼大学,伯尔尼,瑞士),使用视觉(SA1-SA5)和数字(SD_Hue)量表。咀嚼性能的视觉和数字评估具有很强的相关性(Kendall tau = 0.83)。咀嚼能力低定义为 SA 等级 1-2(参考 SA3-SA5)。在调整年龄、性别和临床环境的多变量模型中,我们调查了最大咬合力、牙齿萌出少和支持区少与咀嚼能力低的关系。(3) 结果:平均年龄为 81.9 岁(标准差(SD)5.2),62.9%为女性。总体而言,最大咬合力为 247 N(SD 261)。共有 39 名患者(63.9%)咀嚼功能差,62.9%最大咬合力低,50%牙齿萌出少(<10)。住院和门诊患者的咀嚼性能、萌出牙齿数量和最大咬合力无显著差异。有义齿支持区的数量在门诊患者中明显高于住院患者(中位数 4,四分位距(IQR)4-4;vs. 4,IQR 2-4; = 0.03)。在多变量模型中,最大咬合力和牙齿萌出少与咀嚼能力低独立相关(调整后的比值比 7.4(95%CI,1.8-30.4; < 0.01)和 OR 7.8(95%CI,1.7-36.4; < 0.01))。(4) 结论:欧洲老年住院和门诊患者的口腔功能受损程度相似,均非常普遍。咀嚼能力低与最大咬合力和牙齿萌出少相关,这可能表明基本筛查应包括这些参数中的任何一个,以确定口腔功能受损。