Department of Clinical Biochemistry and Metabolic Medicine, Royal Liverpool University Hospital, Prescot Street, Liverpool L7 8YE, UK.
Department of Musculoskeletal and Ageing Science, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool L7 8TX, UK.
Nutrients. 2024 Aug 15;16(16):2722. doi: 10.3390/nu16162722.
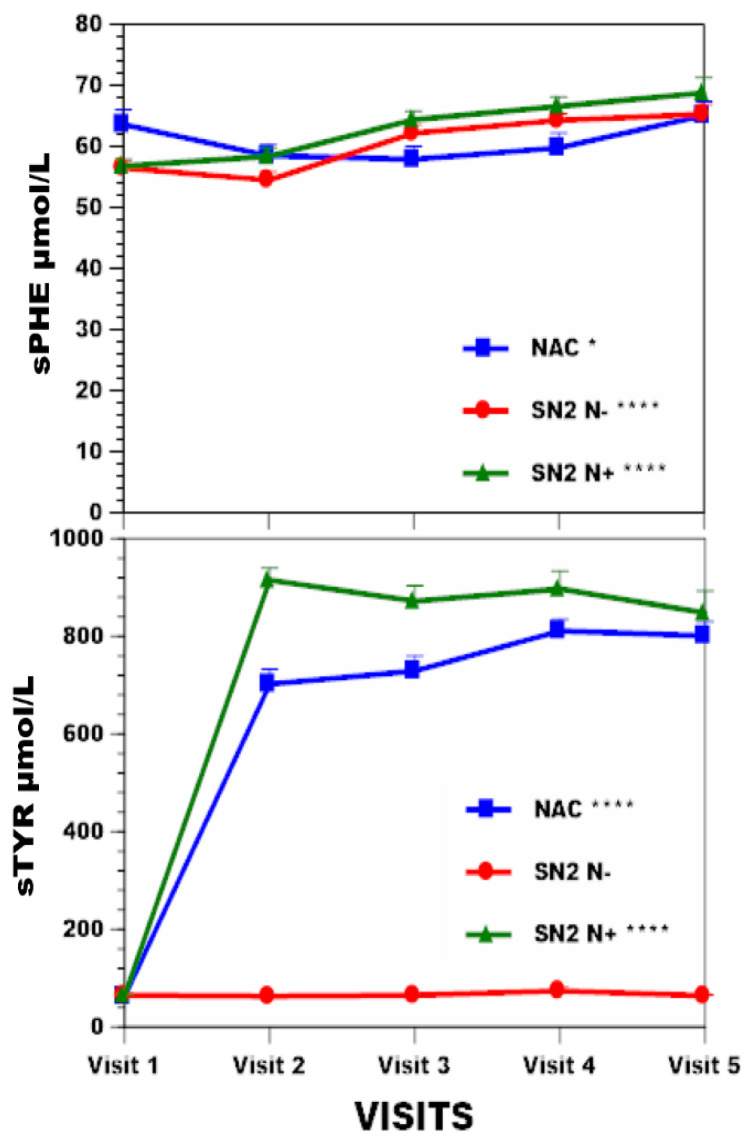
Protein nutrition disorder in alkaptonuria (AKU), resulting in increased homogentisic acid (HGA) before nitisinone therapy and increased tyrosine (TYR) during nitisinone therapy, may benefit from dietetic intervention. The aim of this study was to characterise the diet and their effects prospectively in those who received formal dietetic intervention in the nitisinone-receiving National Alkaptonuria Centre (NAC) patients with those who did not in no-nitisinone Suitability of Nitisinone in Alkaptonuria 2 (SN2 N-) and nitisinone-treated SN2 (SN2 N+) randomised study groups.
A total of 63, 69, and 69 AKU patients from the NAC, SN2 N-, and SN2 N+ were studied for anthropometric (weight, BMI), body composition (including muscle mass, %body fat, hand grip strength), chemical characteristics (serum TYR, serum phenylalanine, urine urea or uUREA, and urine creatinine or uCREAT), and corneal keratopathy. Nitisinone 2 mg and 10 mg were employed in the NAC and SN2 N+ groups, respectively. Dieticians managed protein intake in the NAC, while the SN2 N- and SN2 N+ groups only received advice on self-directed protein restriction during four years of study duration.
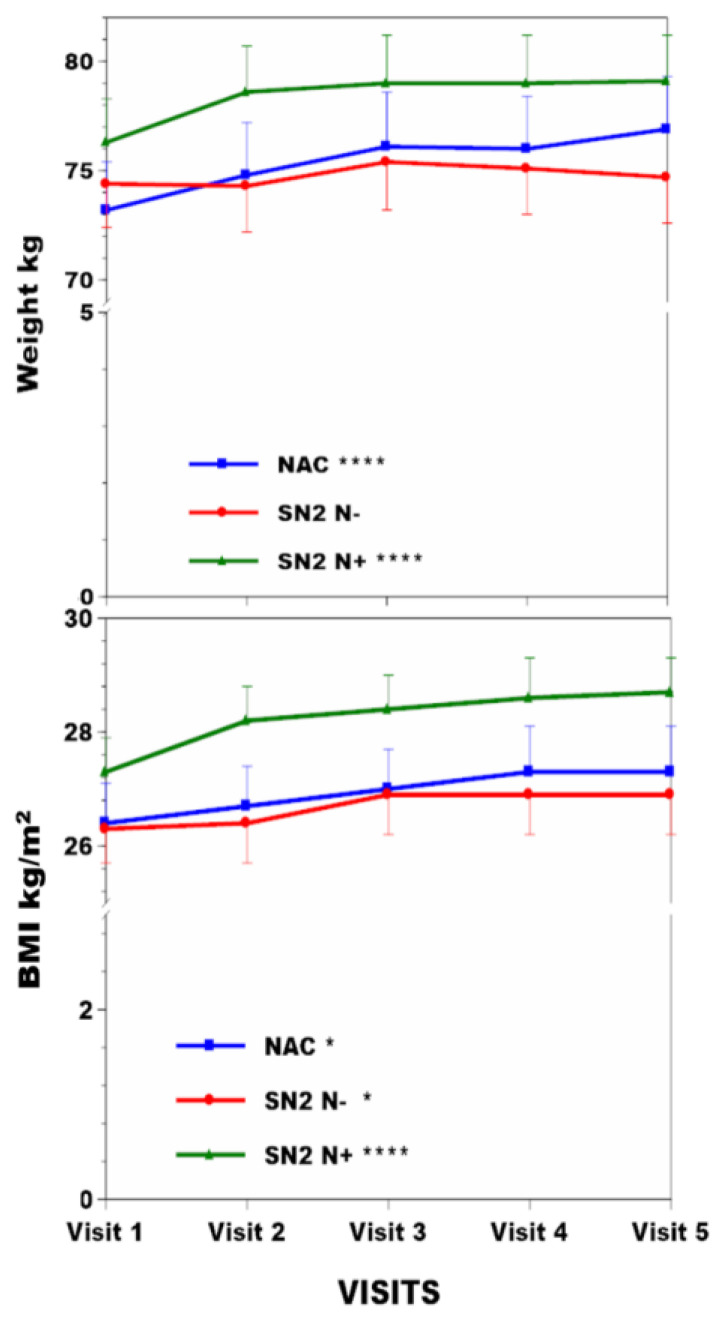
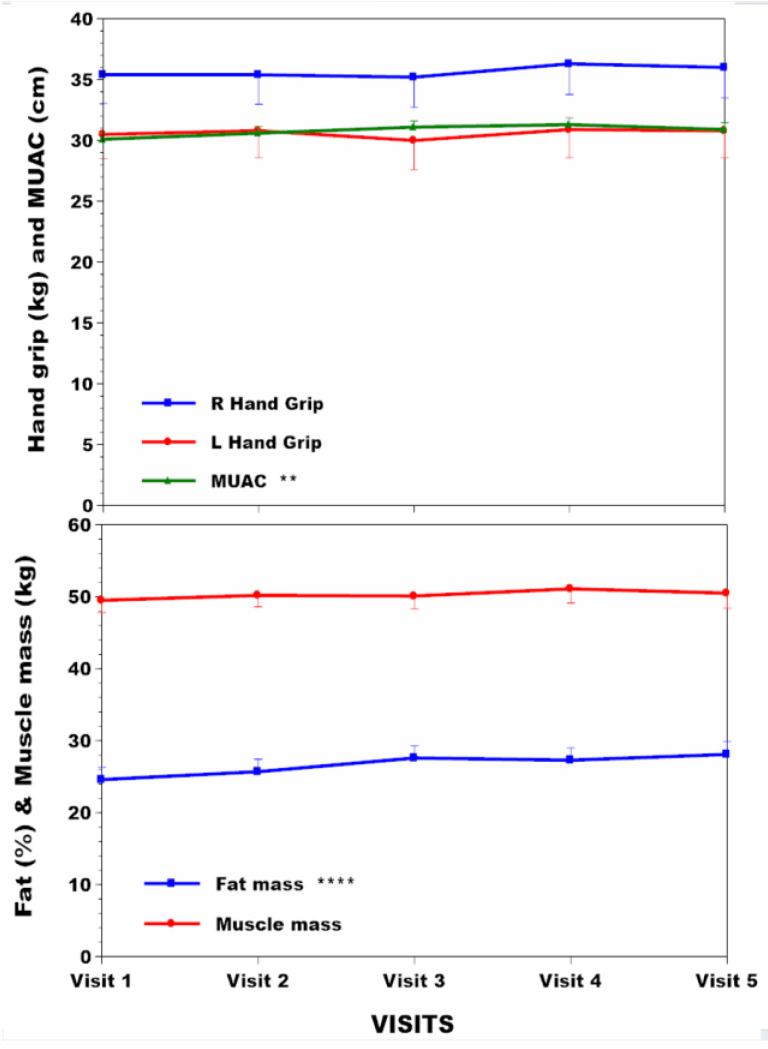
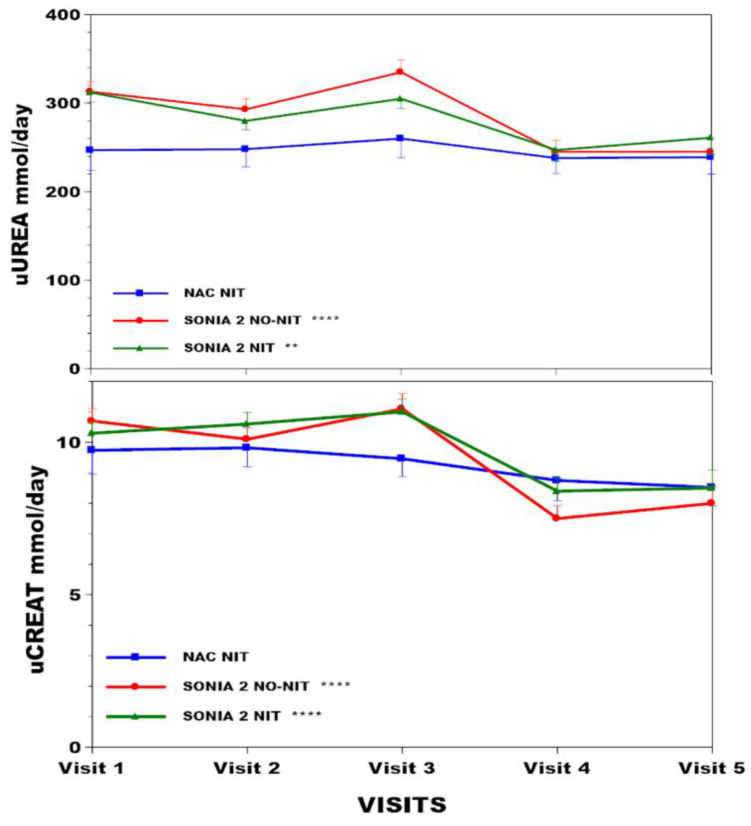
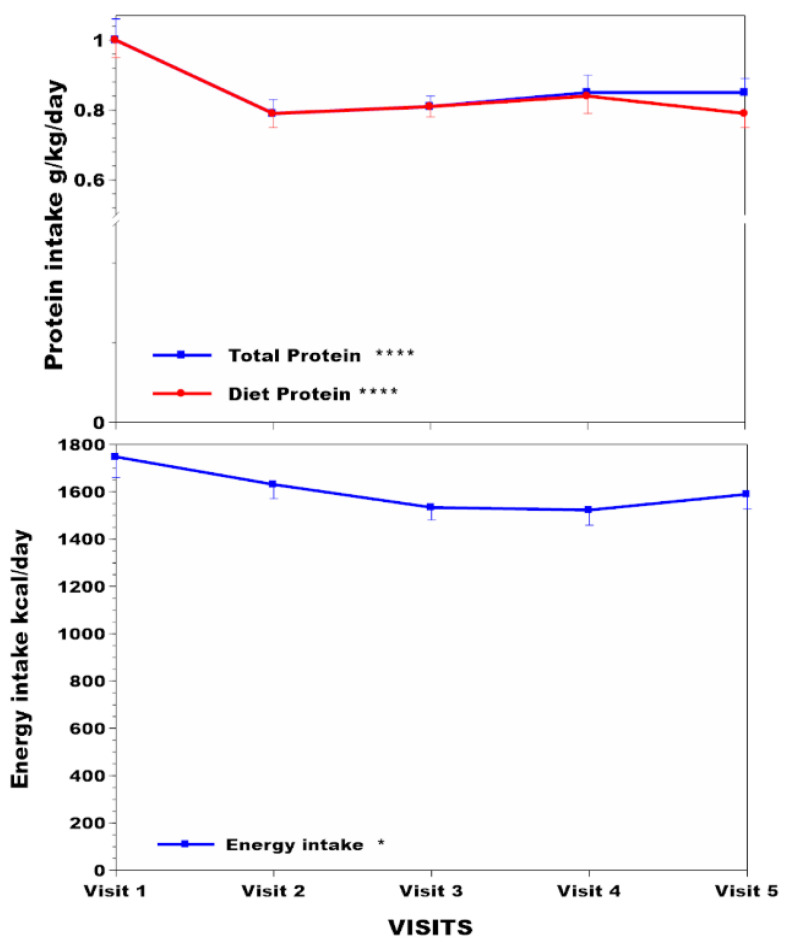
uUREA decreased in the NAC, SN2 N-, and SN2 N+ groups, showing that protein restriction was achieved in these groups. Body weight and BMI increased in the NAC and SN2 N+ groups. uCREAT decreased significantly in SN2 N- and SN2 N+ compared with the NAC over four years of study. Corneal keratopathy was less frequent in the NAC than in the SN2 N+ group. Active dietetic intervention in NAC stabilised lean body mass (muscle mass, hand grip strength) despite a decrease in uUREA and uCREAT, as well as sTYR.
Ongoing dietetic intervention prevented loss of lean body mass despite protein restriction and moderated serum tyrosine increase, leading to less prevalent corneal keratopathy. Protein restriction risks fat mass gain.
由于尼替西农治疗前高同型半胱氨酸(HGA)和尼替西农治疗中酪氨酸(TYR)增加,导致 alkaptonuria(AKU)中的蛋白质营养紊乱,可能受益于饮食干预。本研究的目的是在接受尼替西农治疗的 National Alkaptonuria 中心(NAC)患者中,前瞻性描述接受正式饮食干预的患者的饮食及其效果,并与未接受尼替西农治疗的 No-Nitisinone Suitability of Nitisinone in Alkaptonuria 2(SN2 N-)和接受尼替西农治疗的 SN2 N+随机研究组进行比较。
共对 63、69 和 69 名 AKU 患者进行研究,分别来自 NAC、SN2 N-和 SN2 N+,并进行了人体测量(体重、BMI)、身体成分(包括肌肉量、%体脂、手握力)、化学特征(血清 TYR、血清苯丙氨酸、尿尿素或 uUREA、尿肌酐或 uCREAT)和角膜混浊度检查。NAC 组使用尼替西农 2 mg 和 10 mg,SN2 N+组使用尼替西农 10 mg。营养师管理 NAC 中的蛋白质摄入量,而 SN2 N-和 SN2 N+组仅在研究期间的四年内接受自我指导的蛋白质限制建议。
NAC、SN2 N-和 SN2 N+组的 uUREA 降低,表明这些组实现了蛋白质限制。NAC 和 SN2 N+组的体重和 BMI 增加。与 NAC 相比,SN2 N-和 SN2 N+组在四年的研究中 uCREAT 显著降低。与 SN2 N+组相比,NAC 组的角膜混浊度较少。NAC 中的主动饮食干预稳定了瘦体重(肌肉量、手握力),尽管 uUREA 和 uCREAT 以及 sTYR 下降。
尽管存在蛋白质限制,但持续的饮食干预可防止瘦体重丢失,并适度控制血清酪氨酸升高,从而导致角膜混浊度降低。蛋白质限制会增加脂肪量。