Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, St. Mary's Campus, Norfolk Place, Paddington, London, W2 1PG, UK.
Department of Nutrition, Oslo New University College, Oslo, Norway.
Sci Rep. 2024 Aug 29;14(1):20054. doi: 10.1038/s41598-024-69637-4.
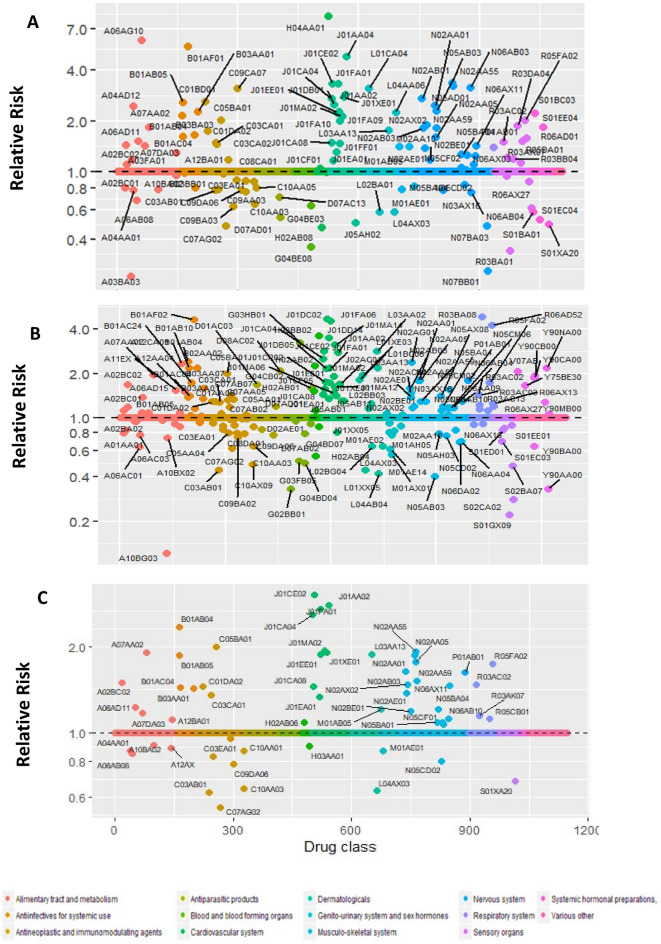
Scandinavian electronic health-care registers provide a unique setting to investigate potential unidentified side effects of drugs. We analysed the association between prescription drugs dispensed in Norway and Sweden and the short-term risk of developing pulmonary embolism. A total of 12,104 pulmonary embolism cases were identified from patient- and cause-of-death registries in Norway (2004-2014) and 36,088 in Sweden (2005-2014). A case-crossover design was used to compare individual drugs dispensed 1-30 days before the date of pulmonary embolism diagnosis with dispensation in a 61-90 day time-window, while controlling for the receipt of other drugs. A BOLASSO approach was used to select drugs that were associated with short-term risk of pulmonary embolism. Thirty-eight drugs were associated with pulmonary embolism in the combined analysis of the Norwegian and Swedish data. Drugs associated with increased risk of pulmonary embolism included certain proton-pump inhibitors, antibiotics, antithrombotics, vasodilators, furosemide, anti-varicose medications, corticosteroids, immunostimulants (pegfilgrastim), opioids, analgesics, anxiolytics, antidepressants, antiprotozoals, and drugs for cough and colds. Mineral supplements, hydrochlorothiazide and potassium-sparing agents, beta-blockers, angiotensin 2 receptor blockers, statins, and methotrexate were associated with lower risk. Most associations persisted, and several additional drugs were associated, with pulmonary embolism when using a longer time window of 90 days instead of 30 days. These results provide exploratory, pharmacopeia-wide evidence of medications that may increase or decrease the risk of pulmonary embolism. Some of these findings were expected based on the drugs' indications, while others are novel and require further study as potentially modifiable precipitants of pulmonary embolism.
斯堪的纳维亚电子医疗登记系统为研究药物潜在的未识别副作用提供了独特的环境。我们分析了挪威和瑞典处方药物的使用与短期肺栓塞风险之间的关联。在挪威(2004-2014 年)的患者和死因登记处共确定了 12104 例肺栓塞病例,在瑞典(2005-2014 年)确定了 36088 例。采用病例交叉设计,将肺栓塞诊断日期前 1-30 天内开出的个体药物与 61-90 天时间窗内开出的药物进行比较,同时控制其他药物的使用。使用 BOLASSO 方法选择与短期肺栓塞风险相关的药物。在对挪威和瑞典数据的联合分析中,有 38 种药物与肺栓塞相关。与肺栓塞风险增加相关的药物包括某些质子泵抑制剂、抗生素、抗血栓药、血管扩张剂、呋塞米、抗静脉曲张药物、皮质类固醇、免疫刺激剂(培非格司亭)、阿片类药物、镇痛药、抗焦虑药、抗抑郁药、抗原生动物药物和咳嗽感冒药。矿物补充剂、氢氯噻嗪和保钾利尿剂、β-受体阻滞剂、血管紧张素 2 受体阻滞剂、他汀类药物和甲氨蝶呤与较低的风险相关。当使用 90 天而不是 30 天的较长时间窗口时,大多数关联仍然存在,并且与肺栓塞相关的另外一些药物也存在关联。这些结果提供了广泛的药物治疗学范围内的探索性证据,表明某些药物可能会增加或降低肺栓塞的风险。其中一些发现基于药物的适应证,而另一些则是新颖的,需要进一步研究,以确定它们是否可能成为肺栓塞的可改变诱因。