Dupraz Chloé, Ducrot Coline, Allignet Benoit, Delpon Gregory, Alexis Anthony, Lapierre Ariane, Supiot Stéphane, Ali David, Piffoux Max
Oncologie médicale, Hospices civils de Lyon, France.
Département de Chirurgie Orthopédique, Hôpital Femme Mère Enfant, Hospices Civils de Lyon, Bron, France.
Clin Transl Radiat Oncol. 2024 Jul 31;48:100834. doi: 10.1016/j.ctro.2024.100834. eCollection 2024 Sep.
The major drivers of carbon dioxide (COeq) emissions of external beam radiation therapy (EBRT) are not well known and limit our ability to initiate mitigation strategies.
We describe the carbon footprint of four typical centers. We explore direct EBRT associated factors such as the impact of fractionation and use of MRI-LINAC, as well as indirect factors (e.g. patient rides). Treatment strategy related COeq emissions are included in a health technology assessment analysis that takes into account COeq emissions.
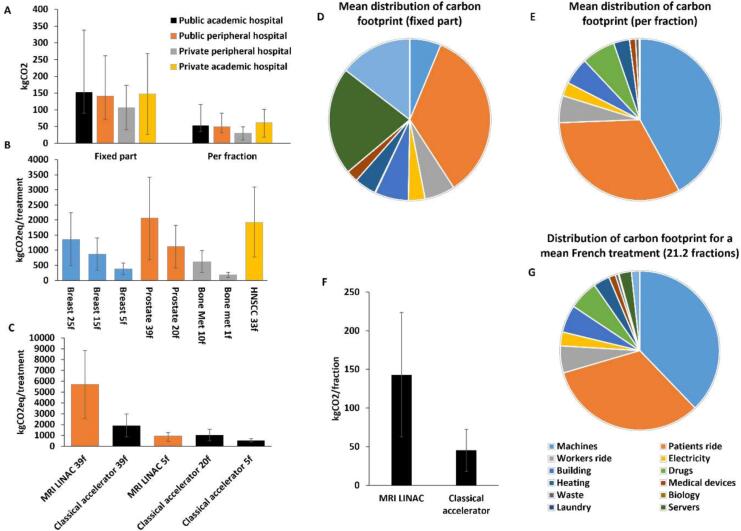
A typical EBRT treatment emits from 185 kgCOeq to 2066 kgCOeq. COeq emissions are mostly driven by (i) accelerator acquisition and maintenance (37.8 %), (ii) patients and workers rides (32.7 %), (iii) drugs and medical devices (7.3 %), (iv) direct energy consumption (6.1 %), and (v) building and bunker construction (5.6 %) with a substantial heterogeneity among centers. Hypofractionation has a strong impact to mitigate emissions. MRI-LINAC is associated with a substantial increase in COeq emissions per fraction and requires ultra hypofractionation in 5 fractions to achieve a similar carbon footprint compared to 20 fractions treatment schemes. The expected limited small increase in toxicities due to hypofractionation (when existing) are in the same range as avoided detrimental effects to future people's health thanks to COeq mitigation.
Carbon footprint of EBRT is not neglectable and could be mitigated. When safely feasible, hypofractionation is one of the main factors to decrease this impact. Taking into account COeq emissions has a substantial impact on the health technology assessment of EBRT, favoring hypofractionated regimens.
外照射放射治疗(EBRT)中二氧化碳(COeq)排放的主要驱动因素尚不明确,这限制了我们制定减排策略的能力。
我们描述了四个典型中心的碳足迹。我们探讨了与EBRT直接相关的因素,如分割方式的影响和MRI直线加速器的使用,以及间接因素(如患者乘车)。与治疗策略相关的COeq排放被纳入一项考虑了COeq排放的卫生技术评估分析中。
一次典型的EBRT治疗排放的COeq为185千克至2066千克。COeq排放主要由以下因素驱动:(i)加速器购置和维护(37.8%),(ii)患者和工作人员乘车(32.7%),(iii)药物和医疗器械(7.3%),(iv)直接能源消耗(6.1%),以及(v)建筑和掩体建设(5.6%),各中心之间存在很大差异。大分割放疗对减排有很大影响。MRI直线加速器与每分次COeq排放的大幅增加相关,与20分次治疗方案相比,需要5分次的超分割放疗才能实现相似的碳足迹。大分割放疗(若存在)导致的毒性预期有限的小幅增加,与因COeq减排对未来人群健康避免的有害影响处于同一范围。
EBRT的碳足迹不可忽视,且可得到缓解。在安全可行的情况下,大分割放疗是降低这种影响的主要因素之一。考虑COeq排放对EBRT的卫生技术评估有重大影响,有利于大分割放疗方案。