Department of Intensive Care, Hospital Israelita Albert Einstein, São Paulo, SP, Brazil.
Department of Anesthesiology, Hospital Israelita Albert Einstein, São Paulo, SP, Brazil.
Crit Care. 2024 Aug 31;28(1):289. doi: 10.1186/s13054-024-05078-9.
Maneuvers assessing fluid responsiveness before an intravascular volume expansion may limit useless fluid administration, which in turn may improve outcomes.
To describe maneuvers for assessing fluid responsiveness in mechanically ventilated patients.
The protocol was registered at PROSPERO: CRD42019146781.
PubMed, EMBASE, CINAHL, SCOPUS, and Web of Science were search from inception to 08/08/2023.
Prospective and intervention studies were selected.
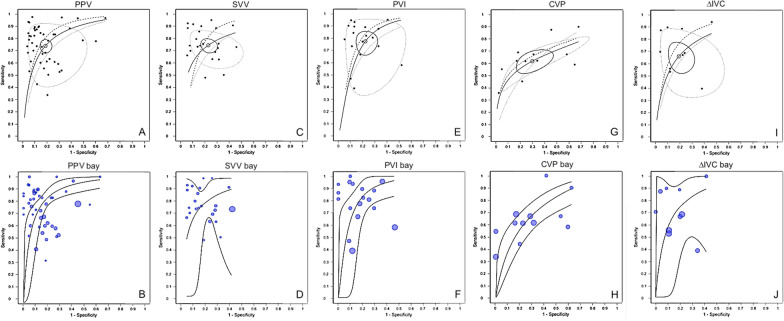
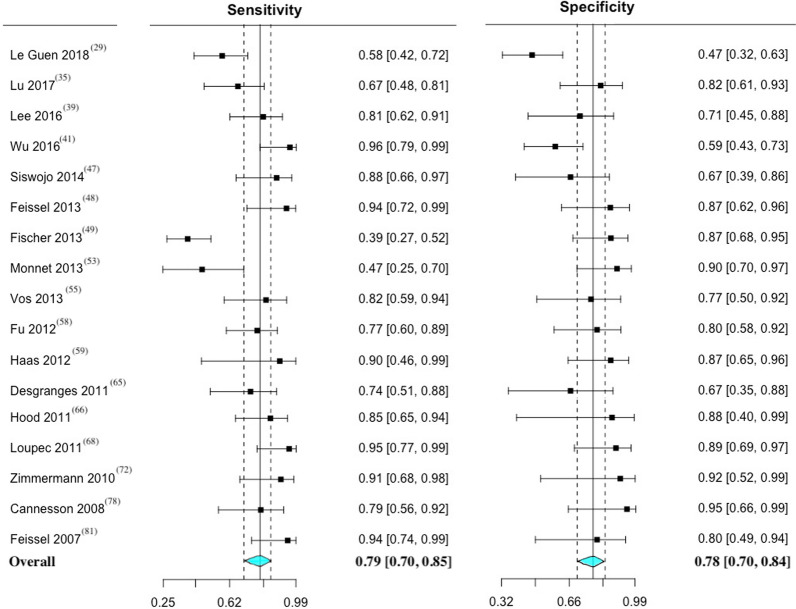
Data for each maneuver were reported individually and data from the five most employed maneuvers were aggregated. A traditional and a Bayesian meta-analysis approach were performed.
A total of 69 studies, encompassing 3185 fluid challenges and 2711 patients were analyzed. The prevalence of fluid responsiveness was 49.9%. Pulse pressure variation (PPV) was studied in 40 studies, mean threshold with 95% confidence intervals (95% CI) = 11.5 (10.5-12.4)%, and area under the receiver operating characteristics curve (AUC) with 95% CI was 0.87 (0.84-0.90). Stroke volume variation (SVV) was studied in 24 studies, mean threshold with 95% CI = 12.1 (10.9-13.3)%, and AUC with 95% CI was 0.87 (0.84-0.91). The plethysmographic variability index (PVI) was studied in 17 studies, mean threshold = 13.8 (12.3-15.3)%, and AUC was 0.88 (0.82-0.94). Central venous pressure (CVP) was studied in 12 studies, mean threshold with 95% CI = 9.0 (7.7-10.1) mmHg, and AUC with 95% CI was 0.77 (0.69-0.87). Inferior vena cava variation (∆IVC) was studied in 8 studies, mean threshold = 15.4 (13.3-17.6)%, and AUC with 95% CI was 0.83 (0.78-0.89).
Fluid responsiveness can be reliably assessed in adult patients under mechanical ventilation. Among the five maneuvers compared in predicting fluid responsiveness, PPV, SVV, and PVI were superior to CVP and ∆IVC. However, there is no data supporting any of the above mentioned as being the best maneuver. Additionally, other well-established tests, such as the passive leg raising test, end-expiratory occlusion test, and tidal volume challenge, are also reliable.
在进行血管内容量扩充之前评估液体反应性的操作可能会限制不必要的液体给予,这反过来可能会改善结果。
描述用于评估机械通气患者液体反应性的操作。
方案在 PROSPERO 中进行了注册:CRD42019146781。
从开始到 2023 年 8 月 08 日,PubMed、EMBASE、CINAHL、SCOPUS 和 Web of Science 进行了搜索。
选择了前瞻性和干预性研究。
单独报告了每个操作的数据,并汇总了使用最多的五个操作的数据。进行了传统和贝叶斯荟萃分析。
共分析了 69 项研究,包括 3185 次液体挑战和 2711 名患者。液体反应性的患病率为 49.9%。脉压变化(PPV)在 40 项研究中进行了研究,95%置信区间(95%CI)的平均阈值为 11.5%(10.5-12.4%),95%CI 的接收者操作特征曲线下面积(AUC)为 0.87(0.84-0.90)。每搏量变异(SVV)在 24 项研究中进行了研究,95%CI 的平均阈值为 12.1%(10.9-13.3%),95%CI 的 AUC 为 0.87(0.84-0.91)。容积描记变异指数(PVI)在 17 项研究中进行了研究,平均阈值为 13.8%(12.3-15.3%),AUC 为 0.88(0.82-0.94)。中心静脉压(CVP)在 12 项研究中进行了研究,95%CI 的平均阈值为 9.0mmHg(7.7-10.1),95%CI 的 AUC 为 0.77(0.69-0.87)。下腔静脉变异(IVC)在 8 项研究中进行了研究,平均阈值为 15.4%(13.3-17.6%),95%CI 的 AUC 为 0.83(0.78-0.89)。
在机械通气的成年患者中,可以可靠地评估液体反应性。在预测液体反应性的五个操作中,PPV、SVV 和 PVI 优于 CVP 和 ∆IVC。然而,没有数据支持上述任何一种操作作为最佳操作。此外,其他经过验证的测试,如被动抬腿试验、呼气末阻断试验和潮气量挑战,也是可靠的。