Myklebust Lena, Monopoli Giulia, Balaban Gabriel, Aabel Eivind Westrum, Ribe Margareth, Castrini Anna Isotta, Hasselberg Nina Eide, Bugge Cecilie, Five Christian, Haugaa Kristina, Maleckar Mary M, Arevalo Hermenegild
Computational Physiology Department, Simula Research Laboratory, Oslo, Norway.
School of Economics Innovation and Technology, Kristiania University College, Oslo, Norway.
Front Physiol. 2024 Aug 19;15:1447938. doi: 10.3389/fphys.2024.1447938. eCollection 2024.
The electrophysiological mechanism connecting mitral valve prolapse (MVP), premature ventricular complexes and life-threatening ventricular arrhythmia is unknown. A common hypothesis is that stretch activated channels (SACs) play a significant role. SACs can trigger depolarizations or shorten repolarization times in response to myocardial stretch. Through these mechanisms, pathological traction of the papillary muscle (PM), as has been observed in patients with MVP, may induce irregular electrical activity and result in reentrant arrhythmia.
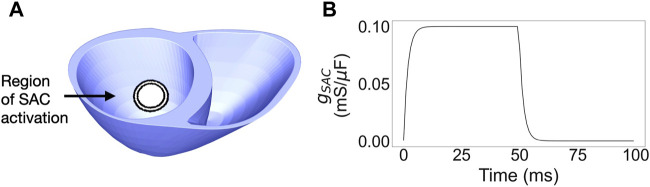
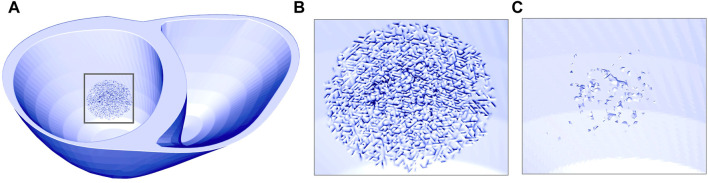
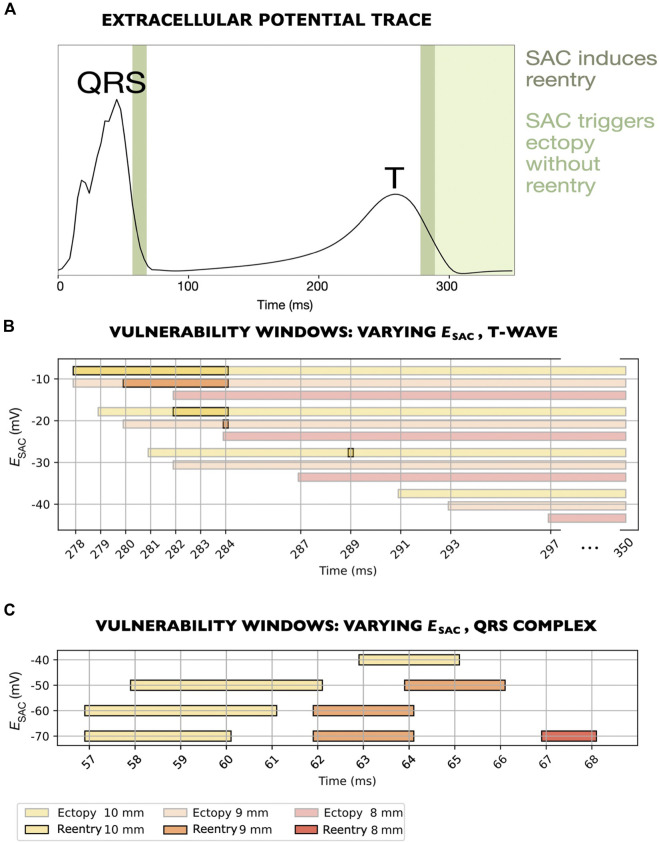
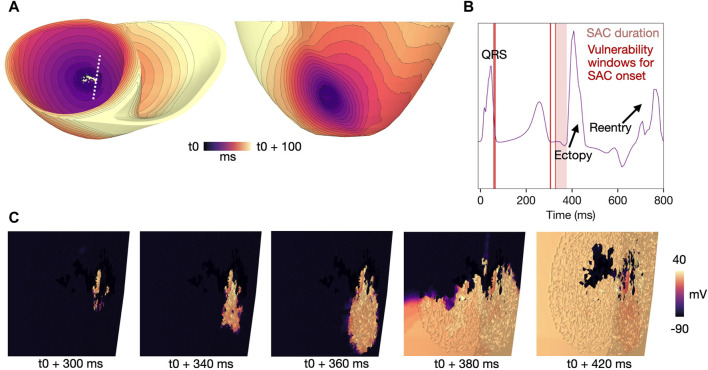
Based on a patient with MVP and mitral annulus disjunction, we modeled the effect of excessive PM traction in a detailed medical image-derived ventricular model by activating SACs in the PM insertion region. By systematically varying the onset of SAC activation following sinus pacing, we identified vulnerability windows for reentry with 1 ms resolution. We explored how reentry was affected by the SAC reversal potential and the size of the region with simulated stretch (SAC region). Finally, the effect of global or focal fibrosis, modeled as reduction in tissue conductivity or mesh splitting (fibrotic microstructure), was investigated.
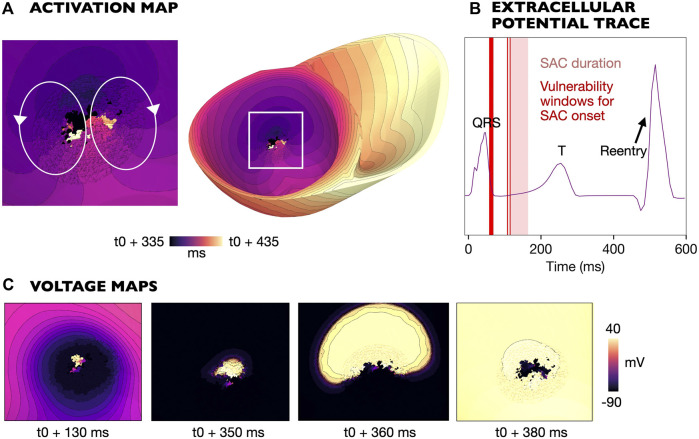
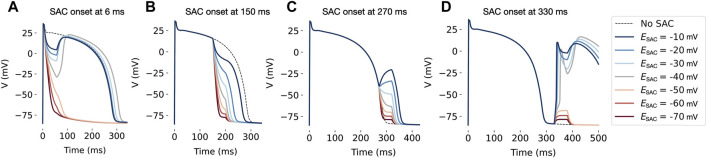
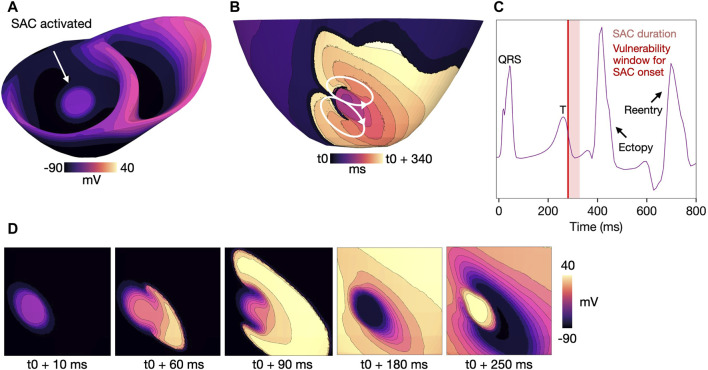
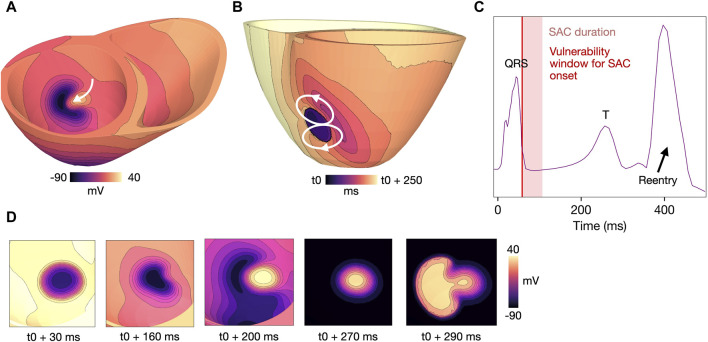
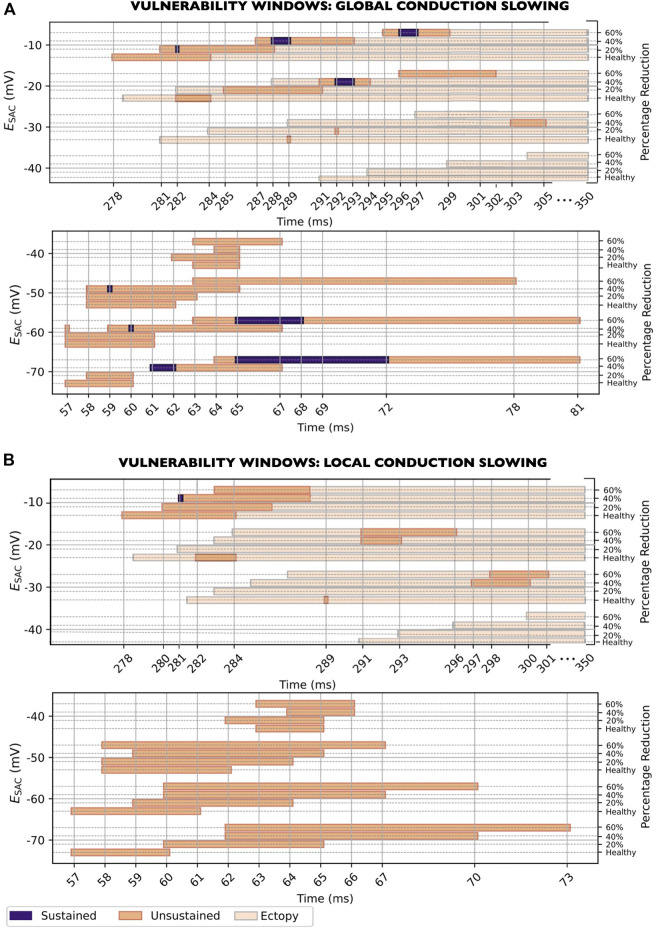
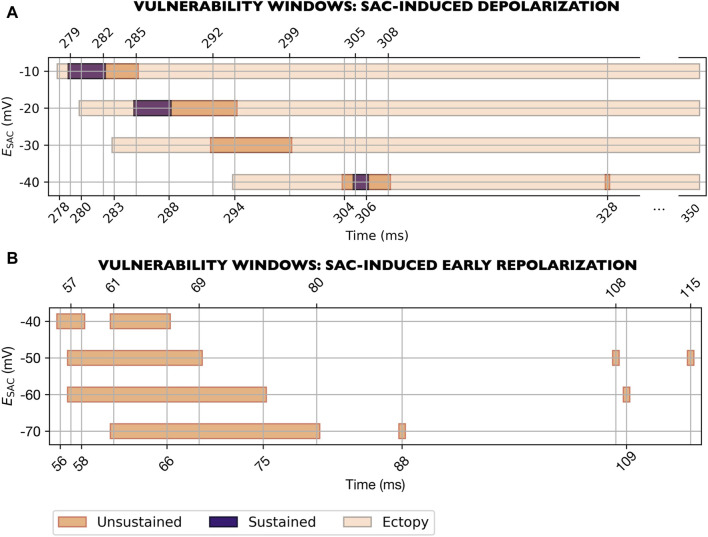
In models with healthy tissue or fibrosis modeled solely as CV slowing, we observed two vulnerable periods of reentry: For of -10 and -30 mV, SAC activated during the T-wave could cause depolarization of the SAC region which lead to reentry. For of -40 and -70 mV, SAC activated during the QRS complex could result in early repolarization of the SAC region and subsequent reentry. In models with fibrotic microstructure in the SAC region, we observed micro-reentries and a larger variability in which times of SAC activation triggered reentry. In these models, 86% of reentries were triggered during the QRS complex or T-wave. We only observed reentry for sufficiently large SAC regions ( 8 mm radius in models with healthy tissue).
Stretch of the PM insertion region following sinus activation may initiate ventricular reentry in patients with MVP, with or without fibrosis. Depending on the SAC reversal potential and timing of stretch, reentry may be triggered by ectopy due to SAC-induced depolarizations or by early repolarization within the SAC region.
二尖瓣脱垂(MVP)、室性早搏与危及生命的室性心律失常之间的电生理机制尚不清楚。一个常见的假说是牵张激活通道(SACs)起重要作用。SACs可响应心肌牵张触发去极化或缩短复极时间。通过这些机制,如在MVP患者中观察到的那样,乳头肌(PM)的病理性牵张可能诱发不规则电活动并导致折返性心律失常。
基于一名患有MVP和二尖瓣环分离的患者,我们通过激活PM插入区域的SACs,在一个详细的源自医学图像的心室模型中模拟了过度PM牵张的影响。通过系统改变窦性起搏后SAC激活的起始时间,我们以1毫秒的分辨率确定了折返的易损窗口。我们探讨了折返如何受SAC反转电位和模拟牵张区域(SAC区域)大小的影响。最后,研究了整体或局灶性纤维化(模拟为组织电导率降低或网格分裂(纤维化微观结构))的影响。
在仅将纤维化模拟为传导速度减慢的健康组织模型中,我们观察到两个折返易损期:对于-10和-30 mV的SAC,在T波期间激活可导致SAC区域去极化,进而导致折返。对于-40和-70 mV的SAC,在QRS复合波期间激活可导致SAC区域早期复极及随后的折返。在SAC区域具有纤维化微观结构的模型中,我们观察到微折返以及SAC激活时间触发折返的更大变异性。在这些模型中,86%的折返在QRS复合波或T波期间触发。我们仅在SAC区域足够大时(健康组织模型中半径≥8毫米)观察到折返。
窦性激活后PM插入区域的牵张可能在有或没有纤维化的MVP患者中引发心室折返。根据SAC反转电位和牵张时间,折返可能由SAC诱导的去极化引起的异位搏动或SAC区域内的早期复极触发。