Department of Medicine, Division of Nephrology, Vagelos College of Physicians & Surgeons, Columbia University, New York, New York, USA.
University of British Columbia, Vancouver, British Columbia, Canada.
J Clin Invest. 2024 Sep 3;134(17):e178573. doi: 10.1172/JCI178573.
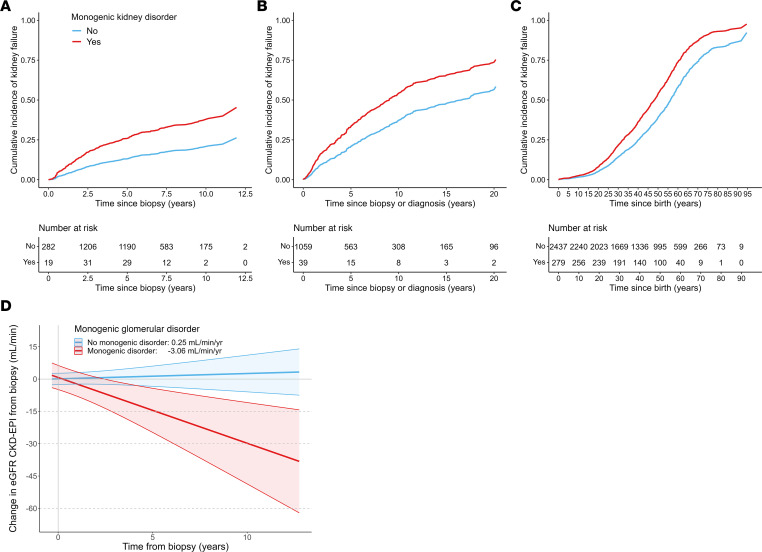
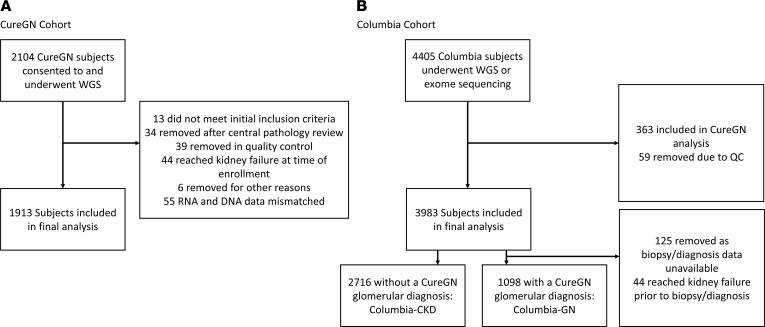
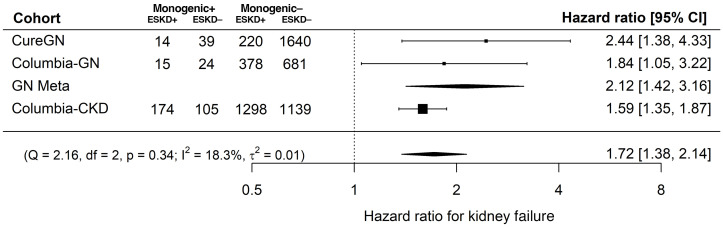
BACKGROUNDIt is unknown whether the risk of kidney disease progression and failure differs between patients with and without genetic kidney disorders.METHODSThree cohorts were evaluated: the prospective Cure Glomerulonephropathy Network (CureGN) and 2 retrospective cohorts from Columbia University, including 5,727 adults and children with kidney disease from any etiology who underwent whole-genome or exome sequencing. The effects of monogenic kidney disorders and APOL1 kidney-risk genotypes on the risk of kidney failure, estimated glomerular filtration rate (eGFR) decline, and disease remission rates were evaluated along with diagnostic yields and the impact of American College of Medical Genetics secondary findings (ACMG SFs).RESULTSMonogenic kidney disorders were identified in 371 patients (6.5%), high-risk APOL1 genotypes in 318 (5.5%), and ACMG SFs in 100 (5.2%). Family history of kidney disease was the strongest predictor of monogenic disorders. After adjustment for traditional risk factors, monogenic kidney disorders were associated with an increased risk of kidney failure (hazard ratio [HR] = 1.72), higher rate of eGFR decline (-3.06 vs. 0.25 mL/min/1.73 m2/year), and lower risk of complete remission (odds ratioNot achieving CR = 5.25). High-risk APOL1 genotypes were associated with an increased risk of kidney failure (HR = 1.67) and faster eGFR decline (-2.28 vs. 0.25 mL/min/1.73 m2), replicating prior findings. ACMG SFs were not associated with personal or family history of associated diseases, but were predicted to impact care in 70% of cases.CONCLUSIONSMonogenic kidney disorders were associated with an increased risk of kidney failure, faster eGFR decline, and lower rates of complete remission, suggesting opportunities for early identification and intervention based on molecular diagnosis.TRIAL REGISTRATIONNA.FUNDINGNational Institute of Diabetes and Digestive and Kidney Diseases grants U24DK100845 (formerly UM1DK100845), U01DK100846 (formerly UM1DK100846), U01DK100876 (formerly UM1DK100876), U01DK100866 (formerly UM1DK100866), U01DK100867 (formerly UM1DK100867), U24DK100845, DK081943, RC2DK116690, 2U01DK100876, 1R01DK136765, 5R01DK082753, and RC2-DK122397; NephCure Kidney International; Department of Defense Research Awards PR201425, W81XWH-16-1-0451, and W81XWH-22-1-0966; National Center for Advancing Translational Sciences grant UL1TR001873; National Library of Medicine grant R01LM013061; National Human Genome Research Institute grant 2U01HG008680.
目前尚不清楚患有和不患有遗传性肾脏疾病的患者的肾脏疾病进展和衰竭风险是否存在差异。
评估了三个队列:前瞻性 Cure Glomerulonephropathy Network (CureGN) 以及来自哥伦比亚大学的两个回顾性队列,包括 5727 名患有任何病因的肾脏疾病的成人和儿童,他们接受了全基因组或外显子组测序。评估了单基因肾脏疾病和 APOL1 肾脏风险基因型对肾衰竭、估计肾小球滤过率(eGFR)下降和疾病缓解率的风险,以及诊断率和美国医学遗传学学院次要发现(ACMG SFs)的影响。
在 371 名患者(6.5%)中发现了单基因肾脏疾病,在 318 名患者(5.5%)中发现了高危 APOL1 基因型,在 100 名患者(5.2%)中发现了 ACMG SFs。肾脏疾病家族史是单基因疾病的最强预测因素。在调整传统危险因素后,单基因肾脏疾病与肾衰竭风险增加相关(风险比 [HR] = 1.72)、eGFR 下降速度更快(-3.06 与 0.25 mL/min/1.73 m2/年)以及完全缓解率降低(比值比未达到 CR = 5.25)。高危 APOL1 基因型与肾衰竭风险增加相关(HR = 1.67)和 eGFR 下降速度加快(-2.28 与 0.25 mL/min/1.73 m2),这与先前的发现一致。ACMG SFs 与相关疾病的个人或家族史无关,但预计在 70%的病例中会影响治疗。
单基因肾脏疾病与肾衰竭风险增加、eGFR 下降速度加快以及完全缓解率降低有关,提示可以根据分子诊断进行早期识别和干预。
无。
美国国立卫生研究院糖尿病、消化和肾脏疾病研究所授予的 U24DK100845(原 UM1DK100845)、U01DK100846(原 UM1DK100846)、U01DK100876(原 UM1DK100876)、U01DK100866(原 UM1DK100866)、U01DK100867(原 UM1DK100867)、U24DK100845、DK081943、RC2DK116690、2U01DK100876、1R01DK136765、5R01DK082753 和 RC2-DK122397;NephCure Kidney International;美国国防部研究奖 PR201425、W81XWH-16-1-0451 和 W81XWH-22-1-0966;国家转化医学科学中心授予的 UL1TR001873;美国国立卫生研究院授予的 R01LM013061;国家人类基因组研究所授予的 2U01HG008680。