Pichon Samuel, Aigrain Pauline, Lacombe Charlotte, Lemarchant Bruno, Ledoult Emmanuel, Koether Vincent, Leurs Amélie, Zebian Ghadi, Launay David, Gachet Benoit, Levy Clémentine
Service de Médecine Interne, Centre de Référence des Maladies Auto-Immunes et Auto-Inflammatoires Systémiques Rares de L'Adulte du Nord, Nord-Ouest, Université de Lille, CHU Lille, Méditerranée et Guadeloupe (CeRAINOM), Pointe-à-Pitre, France.
Pôle de Réanimation, Université de Lille, CHU Lille, 59000, Lille, France.
J Neurol. 2024 Oct;271(10):6514-6525. doi: 10.1007/s00415-024-12660-2. Epub 2024 Sep 3.
Describe the demographic data and clinical phenotype of cranial palsy induced by immune checkpoint inhibitors (CNP-ICI).
A systematic literature review of the literature was performed in Pubmed, Web of Science, and Embase, including 68 articles and 136 patients (PROSPERO no. CRD42024517262).
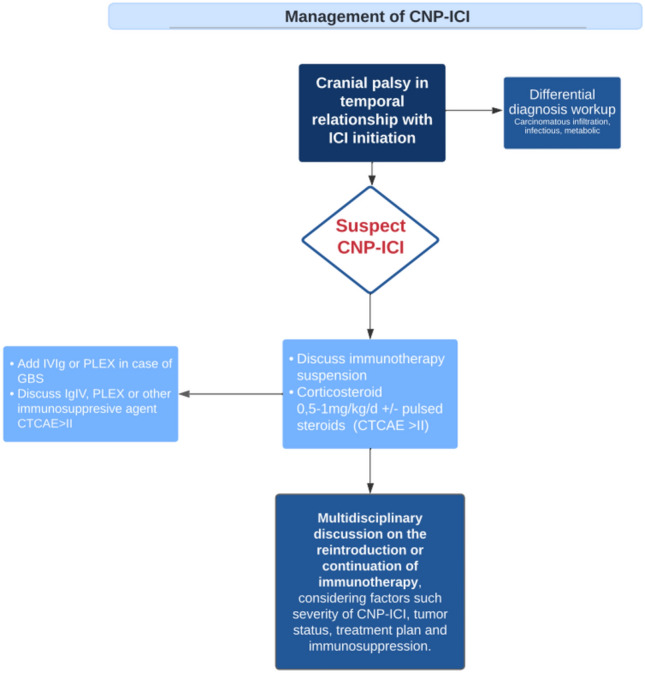
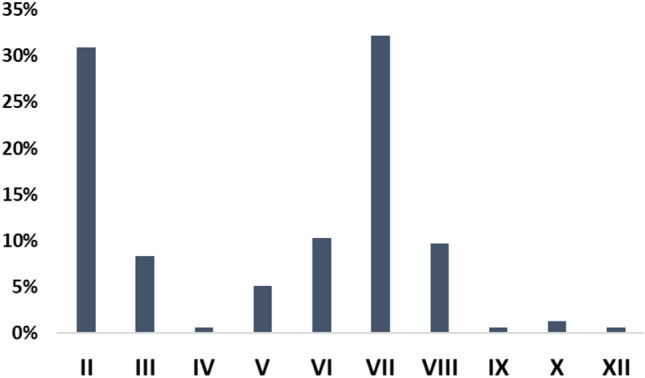
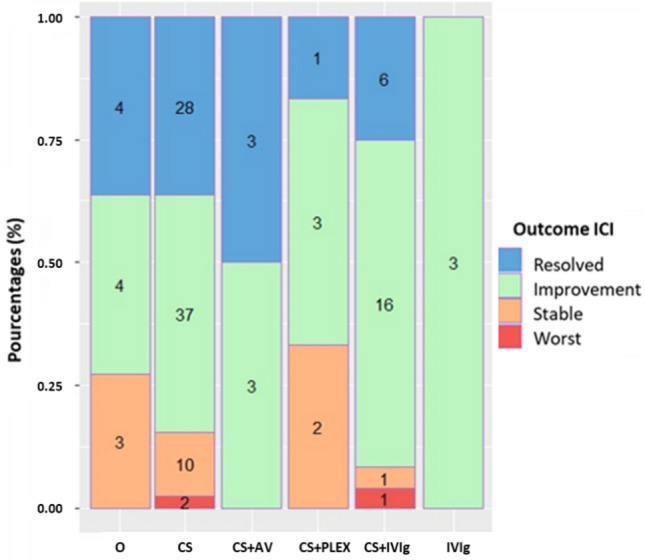
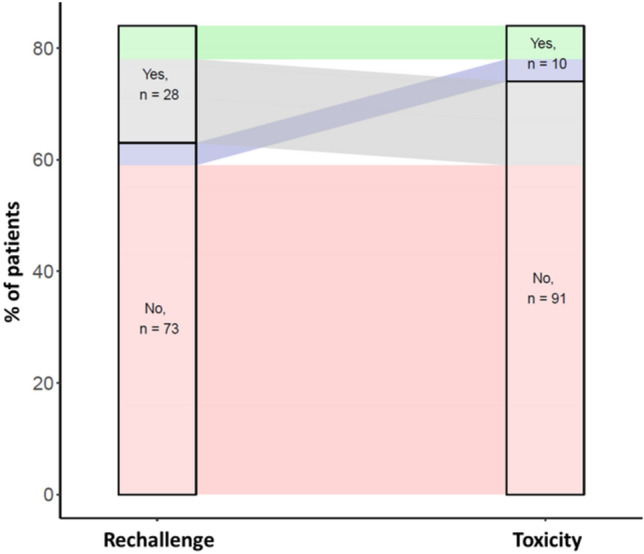
Out of the 1205 articles screened, 68 articles were included after fulfilling the inclusion criteria, for a total of 136 patients. All articles were case reports and case series. In the cohort studied, 52% of patients were treated with anti PD-1/PDL-1 therapies, 14% with anti CTLA-4 therapies, and 34% with a combination of anti CTLA-4 and anti PD-1/PDL-1 therapies. The facial nerve was the most affected cranial nerve, involved in 38% of cases, followed by the optic nerve (35%), the cochleovestibular nerve (12%), and the abducens nerve (10%). The median time from the initial immune checkpoint inhibitor (ICI) injection to the onset CNP-ICI was 10 weeks (IQR 4-20). Magnetic resonance imaging demonstrated contrast enhancement or abnormal signal of the affected nerve in 43% of cases. Cerebrospinal fluid analysis indicated lymphocytic pleocytosis in 59% of cases. At the onset of immune-related adverse events, 89% of patients discontinued immunotherapy, and 92% received treatment for CNP-ICI. Treatment regimens included corticosteroids in 86% of cases, intravenous immunoglobulin in 21%, and plasma exchange in 5.1%. Among the whole population, 33% achieved recovery, 52% showed clinical improvement, 16% remained stable, and 3% experienced worsening of their condition. Rechallenge with immunotherapy was significantly associated with the emergence of new immune-related Adverse Events (irAEs).
ICI therapy may lead to cranial nerve involvement, particularly affecting the facial nerve, typically presenting around 10 weeks after treatment initiation. While corticosteroid therapy often resulted in patient improvement, rechallenging with ICIs were associated with new irAEs.
描述免疫检查点抑制剂所致颅神经麻痹(CNP - ICI)的人口统计学数据和临床表型。
在PubMed、科学网和Embase上对文献进行系统回顾,纳入68篇文章及136例患者(PROSPERO编号:CRD42024517262)。
在筛选的1205篇文章中,68篇符合纳入标准被纳入,共136例患者。所有文章均为病例报告和病例系列。在所研究的队列中,52%的患者接受抗PD - 1/PDL - 1治疗,14%接受抗CTLA - 4治疗,34%接受抗CTLA - 4与抗PD - 1/PDL - 1联合治疗。面神经是受影响最严重的颅神经,38%的病例受累,其次是视神经(35%)、耳蜗前庭神经(12%)和展神经(10%)。从首次注射免疫检查点抑制剂(ICI)到CNP - ICI发病的中位时间为10周(四分位间距4 - 20)。43%的病例磁共振成像显示受累神经有强化或异常信号。脑脊液分析显示59%的病例有淋巴细胞增多。在免疫相关不良事件发生时,89%的患者停止免疫治疗,92%接受了CNP - ICI治疗。治疗方案包括86%的病例使用糖皮质激素,21%使用静脉注射免疫球蛋白,5.1%使用血浆置换。在整个人群中,33%实现康复,52%临床改善,16%病情稳定,3%病情恶化。再次使用免疫治疗与新的免疫相关不良事件(irAEs)的出现显著相关。
ICI治疗可能导致颅神经受累,尤其影响面神经,通常在治疗开始后约10周出现。虽然糖皮质激素治疗常使患者病情改善,但再次使用ICI与新的irAEs相关。