Koss Catherine A, Gandhi Monica, Halvas Elias K, Okochi Hideaki, Chu Carolyn, Glidden David V, Georgetti Gomez Lisa, Heaps Amy L, Conroy Amy A, Tran Michael, Shetler Cory, Hoeth Dianna, Kuncze Karen, Louie Alexander, Rivera Garza Hana, Wafula Mugoma Erick, Penrose Kerri J, Chohan Bhavna H, Ayieko James O, Mills Anthony, Patel Rupa R, Mellors John W, Parikh Urvi M
University of California, San Francisco, San Francisco, California, USA.
University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
Open Forum Infect Dis. 2024 Aug 26;11(9):ofae468. doi: 10.1093/ofid/ofae468. eCollection 2024 Sep.
Long-acting cabotegravir (CAB-LA) is highly effective for HIV prevention, but delayed HIV diagnoses and integrase strand transfer inhibitor (INSTI) resistance were observed in trials. We report the first case in routine clinical care of HIV infection on CAB-LA with INSTI resistance.
The SeroPrEP study enrolls individuals in the United States who acquire HIV on pre-exposure prophylaxis modalities to assess diagnostics, antiretroviral (ARV) drug levels, resistance, and treatment outcomes. Resistance mutations in full-length HIV-1 integrase were identified by single-genome sequencing (SGS). Cabotegravir concentrations in plasma and hair segments were measured by liquid chromatography-tandem mass spectrometry.
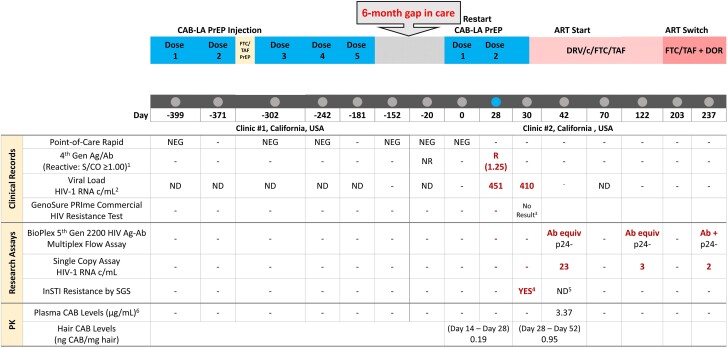
A 23-year-old gender-nonbinary person, male at birth, restarted CAB-LA 6 months after discontinuation due to losing insurance. Prior to restart, HIV-1 RNA was not detected, but 20 days elapsed before CAB-LA injection. After the second CAB-LA injection, HIV antigen/antibody returned reactive (HIV-1 RNA 451 copies/mL). SGS of plasma HIV-1 RNA identified INSTI mutation Q148R in 2/24 sequences 2 days postdiagnosis; commercial genotype failed amplification. Cabotegravir hair concentration was 0.190 ng/mg 2 weeks prediagnosis; plasma cabotegravir was high (3.37 μg/mL; ∼20× PA-IC) 14 days postdiagnosis. Viral suppression was maintained for 6 months on darunavir/cobicistat/emtricitabine/tenofovir alafenamide, then switched to doravirine + emtricitabine/tenofovir alafenamide due to nausea.
In this first case of HIV infection on CAB-LA with INSTI resistance in routine care, cabotegravir resistance was detected only with a sensitive research assay. Accelerated pathways to minimize time between HIV testing and CAB-LA initiation are needed to optimize acute HIV detection and mitigate resistance risk. Sustained product access regardless of insurance is imperative to reduce HIV infections on CAB-LA.
长效卡博特韦(CAB-LA)对预防HIV非常有效,但在试验中观察到HIV诊断延迟和整合酶链转移抑制剂(INSTI)耐药情况。我们报告了首例在接受CAB-LA治疗时出现INSTI耐药的HIV感染常规临床病例。
SeroPrEP研究招募了美国采用暴露前预防模式感染HIV的个体,以评估诊断、抗逆转录病毒(ARV)药物水平、耐药性和治疗结果。通过单基因组测序(SGS)鉴定全长HIV-1整合酶中的耐药突变。采用液相色谱-串联质谱法测定血浆和毛发段中的卡博特韦浓度。
一名23岁的出生时为男性的非二元性别者,因失去保险在停药6个月后重新开始使用CAB-LA。重新开始用药前未检测到HIV-1 RNA,但在注射CAB-LA前间隔了20天。第二次注射CAB-LA后,HIV抗原/抗体呈反应性(HIV-1 RNA 451拷贝/mL)。诊断后2天,血浆HIV-1 RNA的SGS在2/24个序列中鉴定出INSTI突变Q148R;商业基因分型未能扩增。诊断前2周卡博特韦毛发浓度为0.190 ng/mg;诊断后14天血浆卡博特韦水平较高(3.37 μg/mL;约为预测活性浓度的2�倍)。使用达芦那韦/考比司他/恩曲他滨/替诺福韦艾拉酚胺维持病毒抑制6个月,随后因恶心改用多拉韦林+恩曲他滨/替诺福韦艾拉酚胺。
在这例常规护理中接受CAB-LA治疗且出现INSTI耐药的首例HIV感染病例中,仅通过灵敏的研究检测方法才检测到卡博特韦耐药。需要加快流程以尽量缩短HIV检测与开始使用CAB-LA之间的时间,以优化急性HIV检测并降低耐药风险。无论保险情况如何,持续获得药物对于减少CAB-LA使用者中的HIV感染至关重要。