Mihailescu Sylvia, Hlava Quinn, Cook Philip A, Mandelli Maria Luisa, Lee Suzee E, Boeve Bradley F, Dickerson Bradford C, Gorno-Tempini Maria Luisa, Rogalski Emily, Grossman Murray, Gee James, McMillan Corey T, Olm Christopher A
School of Engineering and Applied Sciences, University of Pennsylvania, Philadelphia, PA, United States.
Department of Neurology, University of Pennsylvania, Philadelphia, PA, United States.
Front Neurol. 2024 Aug 21;15:1452944. doi: 10.3389/fneur.2024.1452944. eCollection 2024.
Frontotemporal lobar degeneration (FTLD) is associated with FTLD due to tau (FTLD-tau) or TDP (FTLD-TDP) inclusions found at autopsy. Arterial Spin Labeling (ASL) MRI is often acquired in the same session as a structural T1-weighted image (T1w), enabling detection of regional changes in cerebral blood flow (CBF). We hypothesize that ASL-T1w registration with more degrees of freedom using boundary-based registration (BBR) will better align ASL and T1w images and show increased sensitivity to regional hypoperfusion differences compared to manual registration in patient participants. We hypothesize that hypoperfusion will be associated with a clinical measure of disease severity, the FTLD-modified clinical dementia rating scale sum-of-boxes (FTLD-CDR).
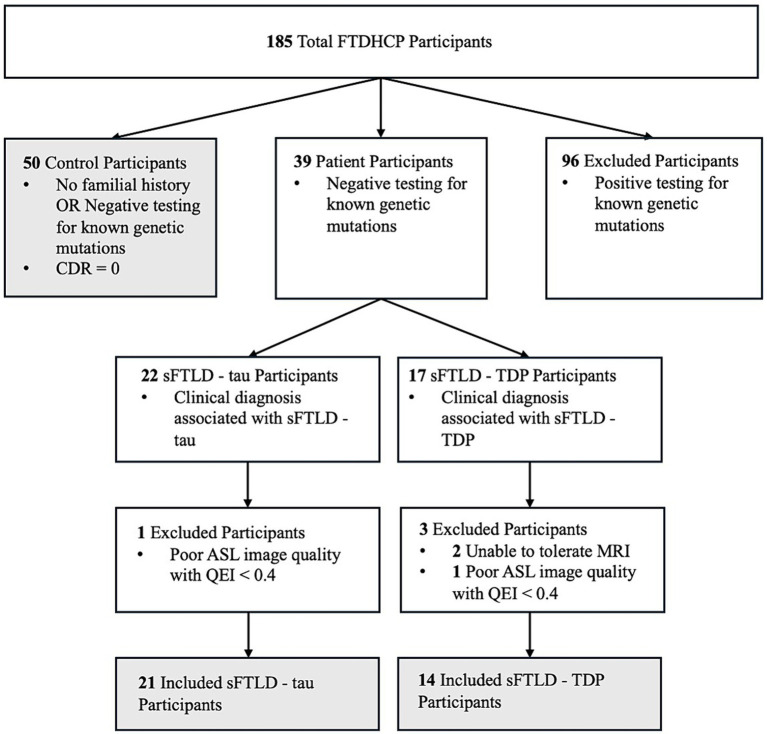
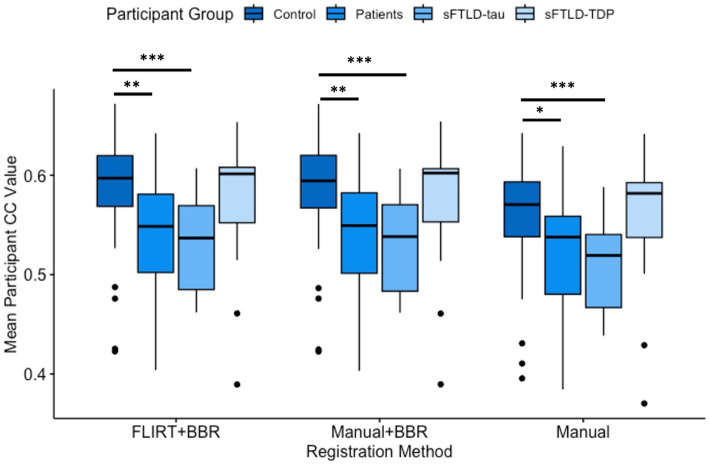
Patients with sporadic likely FTLD-tau (sFTLD-tau; = 21), with sporadic likely FTLD-TDP (sFTLD-TDP; = 14), and controls ( = 50) were recruited from the Connectomic Imaging in Familial and Sporadic Frontotemporal Degeneration project (FTDHCP). Pearson's Correlation Coefficients (CC) were calculated on cortical vertex-wise CBF between each participant for each of 3 registration methods: (1) manual registration, (2) BBR initialized with manual registration (manual+BBR), (3) and BBR initialized using FLIRT (FLIRT+BBR). Mean CBF was calculated in the same regions of interest (ROIs) for each registration method after image alignment. Paired -tests of CC values for each registration method were performed to compare alignment. Mean CBF in each ROI was compared between groups using -tests. Differences were considered significant at < 0.05 (Bonferroni-corrected). We performed linear regression to relate FTLD-CDR to mean CBF in patients with sFTLD-tau and sFTLD-TDP, separately ( < 0.05, uncorrected).
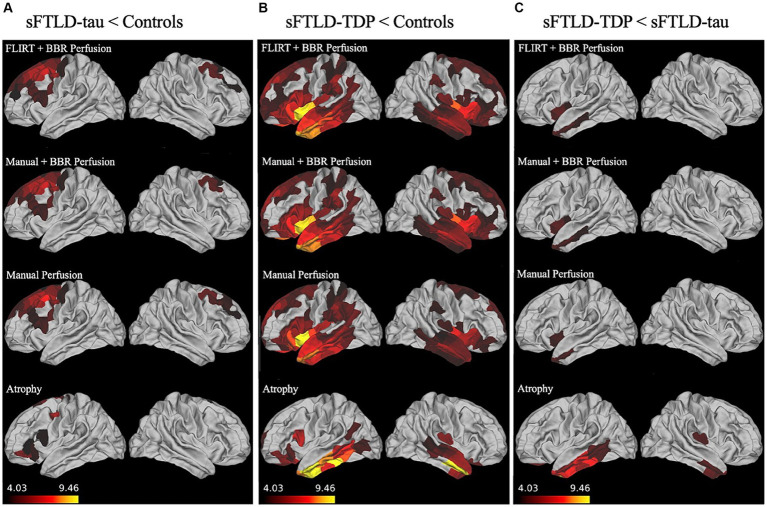
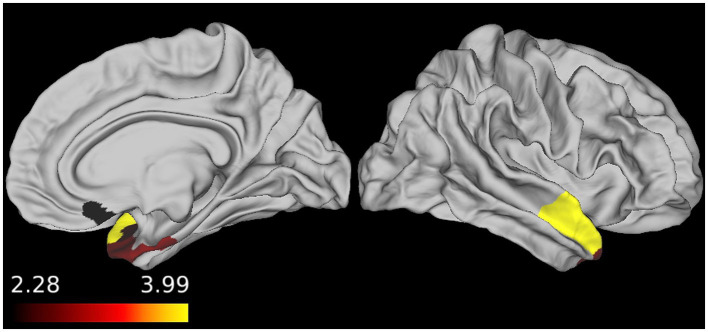
All registration methods demonstrated significant hypoperfusion in frontal and temporal regions in each patient group relative to controls. All registration methods detected hypoperfusion in the left insular cortex, middle temporal gyrus, and temporal pole in sFTLD-TDP relative to sFTLD-tau. FTLD-CDR had an inverse association with CBF in right temporal and orbitofrontal ROIs in sFTLD-TDP. Manual+BBR performed similarly to FLIRT+BBR.
ASL is sensitive to distinct regions of hypoperfusion in patient participants relative to controls, and in patients with sFTLD-TDP relative to sFTLD-tau, and decreasing perfusion is associated with increasing disease severity, at least in sFTLD-TDP. BBR can register ASL-T1w images adequately for controls and patients.
额颞叶变性(FTLD)与尸检时发现的tau蛋白(FTLD-tau)或TDP(FTLD-TDP)包涵体相关。动脉自旋标记(ASL)MRI通常与结构T1加权图像(T1w)在同一时段采集,能够检测脑血流量(CBF)的区域变化。我们假设,与手动配准相比,使用基于边界的配准(BBR)进行具有更多自由度的ASL-T1w配准,将能更好地对齐ASL和T1w图像,并对患者参与者区域灌注不足差异显示出更高的敏感性。我们假设灌注不足将与疾病严重程度的临床指标——FTLD改良临床痴呆评定量表总分(FTLD-CDR)相关。
从家族性和散发性额颞叶变性项目(FTDHCP)的连接组成像研究中招募了散发性可能为FTLD-tau的患者(sFTLD-tau;n = 21)、散发性可能为FTLD-TDP的患者(sFTLD-TDP;n = 14)和对照组(n = 50)。针对三种配准方法中的每一种,计算每个参与者之间皮质顶点处CBF的Pearson相关系数(CC):(1)手动配准,(2)以手动配准初始化的BBR(手动+BBR),(3)使用FLIRT初始化的BBR(FLIRT+BBR)。图像对齐后,针对每种配准方法在相同的感兴趣区域(ROI)计算平均CBF。对每种配准方法的CC值进行配对t检验以比较对齐情况。使用t检验比较各组中每个ROI的平均CBF。差异在p < 0.05(Bonferroni校正)时被认为具有统计学意义。我们分别对sFTLD-tau和sFTLD-TDP患者进行线性回归,以将FTLD-CDR与平均CBF相关联(p < 0.05,未校正)。
相对于对照组,所有配准方法在每个患者组的额叶和颞叶区域均显示出明显的灌注不足。相对于sFTLD-tau,所有配准方法均检测到sFTLD-TDP患者的左侧岛叶皮质、颞中回和颞极存在灌注不足。在sFTLD-TDP患者中,FTLD-CDR与右侧颞叶和眶额ROI中的CBF呈负相关。手动+BBR的表现与FLIRT+BBR相似。
相对于对照组,ASL对患者参与者中不同的灌注不足区域敏感,相对于sFTLD-tau患者,对sFTLD-TDP患者也敏感,并且灌注减少与疾病严重程度增加相关,至少在sFTLD-TDP中如此。BBR能够为对照组和患者充分配准ASL-T1w图像。