Kao Szu-Yu Zoe, Sangha Kinpritma, Fujiwara Naoto, Hoshida Yujin, Parikh Neehar D, Singal Amit G
Siemens Medical Solutions USA Inc., Malvern, PA, USA.
Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX, USA.
EClinicalMedicine. 2024 Aug 13;75:102755. doi: 10.1016/j.eclinm.2024.102755. eCollection 2024 Sep.
Hepatocellular carcinoma (HCC) surveillance is currently performed using a one-size-fits-all strategy with ultrasound plus AFP (US + AFP). There is increasing interest in risk-stratified and precision surveillance strategies incorporating individual risk and variance in surveillance test performance; however, the cost-effectiveness of these approaches has not been evaluated.
We conducted a cost-effectiveness analysis to evaluate four surveillance strategies (no surveillance, universal US + AFP surveillance, risk-stratified surveillance, and precision surveillance) in a simulated cohort of 50-year-old patients with compensated cirrhosis. The most cost-effective strategy was that with the highest incremental cost-effectiveness ratio (ICER) and below the willingness-to-pay (WTP) threshold of $150,000/QALY gained. Model inputs were based on literature review, and costs were derived from the Medicare fee schedule.
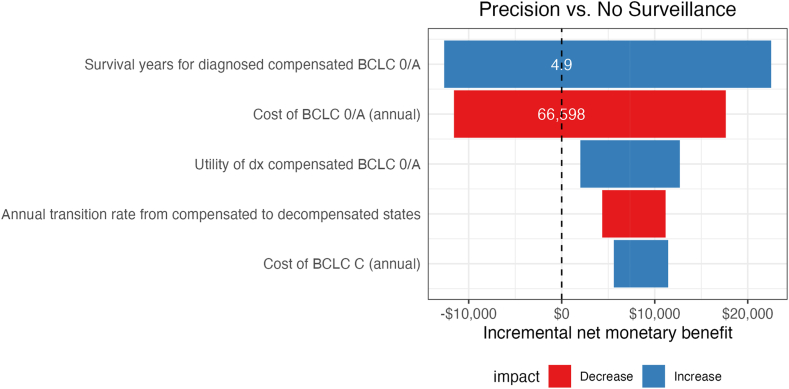
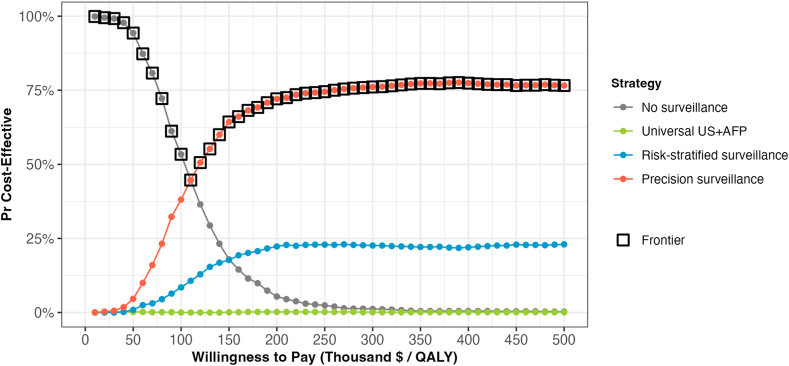
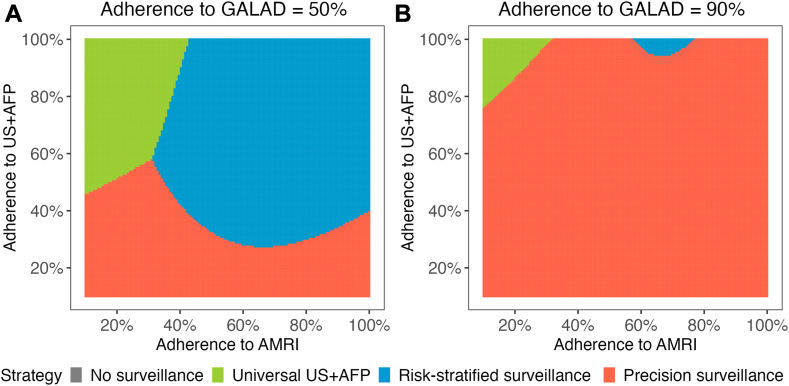
The precision surveillance strategy demonstrated variation in recommended surveillance test based on HCC risk category and patient factors. US + AFP, risk-stratified, and precision surveillance detected more HCC cases per 100,000 population than no surveillance, with a higher proportion of early-stage cases for precision surveillance (67.6%) than risk-stratified (63.8%), universal ultrasound (63.2%), and no surveillance (38.0%). Compared to no surveillance, precision surveillance was most cost-effective, with an ICER of $104,614/QALY gained, whereas US + AFP and risk-stratified surveillance were both dominated. Compared to US + AFP, risk-stratified surveillance was cost saving and dominated US + AFP, whereas precision surveillance was cost-effective, with an ICER of $98,103/QALY gained. Results were sensitive to survival with early-stage HCC, cost of early-stage HCC treatment, and surveillance utilization. Precision surveillance remained the most cost-effective when WTP thresholds exceeded $110,000/QALY gained.
A precision surveillance strategy is the most cost-effective method for HCC surveillance. This approach could maximize surveillance benefits in high-risk patients, while minimizing surveillance harms in low-risk individuals.
National Cancer Institute (U01 CA230694, R01 CA222900, R01 CA212008, and U24ca086368) and Cancer Prevention Research Institute of Texas (CPRIT) (RP200554).
目前肝细胞癌(HCC)监测采用超声联合甲胎蛋白(US + AFP)的“一刀切”策略。人们对纳入个体风险和监测检测性能差异的风险分层及精准监测策略的兴趣与日俱增;然而,这些方法的成本效益尚未得到评估。
我们进行了一项成本效益分析,以评估在一个模拟的50岁代偿期肝硬化患者队列中四种监测策略(不监测、普遍的US + AFP监测、风险分层监测和精准监测)。最具成本效益的策略是增量成本效益比(ICER)最高且低于每获得一个质量调整生命年(QALY)支付意愿(WTP)阈值150,000美元的策略。模型输入基于文献综述,成本来自医疗保险费用表。
精准监测策略根据HCC风险类别和患者因素显示出推荐监测检测的差异。与不监测相比,US + AFP、风险分层和精准监测每10万人口中检测到的HCC病例更多,精准监测的早期病例比例(67.6%)高于风险分层(63.8%)、普遍超声(63.2%)和不监测(38.0%)。与不监测相比,精准监测最具成本效益,ICER为每获得一个QALY 104,614美元,而US + AFP和风险分层监测均被主导。与US + AFP相比,风险分层监测节省成本且主导US + AFP,而精准监测具有成本效益,ICER为每获得一个QALY 98,103美元。结果对早期HCC的生存率、早期HCC治疗成本和监测利用率敏感。当WTP阈值超过每获得一个QALY 110,000美元时,精准监测仍然是最具成本效益的。
精准监测策略是HCC监测最具成本效益的方法。这种方法可以在高风险患者中最大化监测益处,同时在低风险个体中最小化监测危害。
美国国立癌症研究所(U01 CA230694、R01 CA222900、R01 CA212008和U24ca086368)以及德克萨斯州癌症预防与研究机构(CPRIT)(RP200554)。