Department of Anesthesia, Critical Care and Pain Medicine Massachusetts General Hospital, Harvard Medical School Boston MA.
Medical Biodynamics Program, Division of Sleep and Circadian Disorders Brigham and Womens Hospital Boston MA.
J Am Heart Assoc. 2024 Sep 17;13(18):e032086. doi: 10.1161/JAHA.123.032086. Epub 2024 Sep 5.
Many disease processes are influenced by circadian clocks and display ~24-hour rhythms. Whether disruptions to these rhythms increase stroke risk is unclear. We evaluated the association between 24-hour rest-activity rhythms, stroke risk, and major poststroke adverse outcomes.
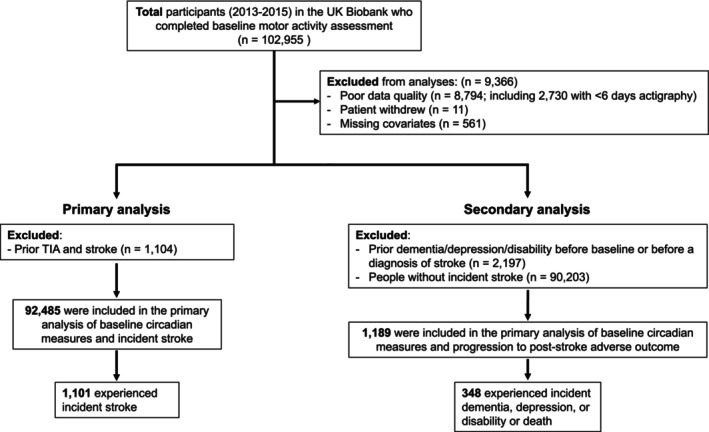
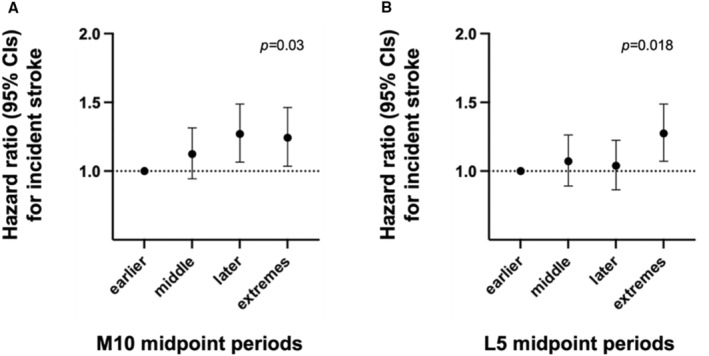
We examined ~100 000 participants from the UK Biobank (aged 44-79 years; ~57% women) assessed with actigraphy (6-7 days) and 5-year median follow-up. We derived (1) most active 10-hour activity counts across the 24-hour cycle and the timing of its midpoint timing; (2) the least active 5-hour count and its midpoint; (3) relative amplitude; (4) interdaily stability; and (5) intradaily variability, for stability and fragmentation of the rhythm. Cox proportional hazard models were constructed for time to (1) incident stroke (n=1652) and (2) poststroke adverse outcomes (dementia, depression, disability, or death). Suppressed relative amplitude (lowest quartile [quartile 1] versus the top quartile [quartile 4]) was associated with stroke risk (hazard ratio [HR], 1.61 [95% CI, 1.35-1.92]; <0.001) after adjusting for demographics. Later most active 10-hour activity count midpoint timing (14:00-15:26; HR, 1.26 [95% CI, 1.07-1.49]; =0.007) also had higher stroke risk than earlier (12:17-13:10) participants. A fragmented rhythm (intradaily variability) was also associated with higher stroke risk (quartile 4 versus quartile 1; HR, 1.26 [95% CI, 1.06-1.49]; =0.008). Suppressed relative amplitude was associated with risk for poststroke adverse outcomes (quartile 1 versus quartile 4; HR, 2.02 [95% CI, 1.46-2.48]; <0.001). All associations were independent of age, sex, race, obesity, sleep disorders, cardiovascular diseases or risks, and other comorbidity burdens.
Suppressed 24-hour rest-activity rhythm may be a risk factor for stroke and an early indicator of major poststroke adverse outcomes.
许多疾病过程受生物钟影响,并呈现出约 24 小时的节律。这些节律的破坏是否会增加中风风险尚不清楚。我们评估了 24 小时休息-活动节律与中风风险以及主要中风后不良结局之间的关系。
我们对来自英国生物库的约 10 万名参与者(年龄 44-79 岁;约 57%为女性)进行了评估,使用活动记录仪(6-7 天)和 5 年的中位随访时间。我们得出了(1)24 小时周期内最活跃的 10 小时活动计数及其中点时间;(2)最不活跃的 5 小时计数及其中点;(3)相对振幅;(4)日间稳定性;以及(5)节律稳定性和碎片化的日内可变性。构建 Cox 比例风险模型来预测时间到(1)首发中风(n=1652)和(2)中风后不良结局(痴呆、抑郁、残疾或死亡)的发生。与最高四分位(四分位 4)相比,抑制的相对振幅(最低四分位[四分位 1])与中风风险相关(风险比[HR],1.61[95%CI,1.35-1.92];<0.001),调整了人口统计学因素。较晚的最活跃 10 小时活动计数中点时间(14:00-15:26;HR,1.26[95%CI,1.07-1.49];=0.007)也比更早(12:17-13:10)的参与者有更高的中风风险。节律碎片化(日内可变性)也与更高的中风风险相关(四分位 4 与四分位 1;HR,1.26[95%CI,1.06-1.49];=0.008)。抑制的相对振幅与中风后不良结局的风险相关(四分位 1 与四分位 4;HR,2.02[95%CI,1.46-2.48];<0.001)。所有关联均独立于年龄、性别、种族、肥胖、睡眠障碍、心血管疾病或风险以及其他合并症负担。
抑制的 24 小时休息-活动节律可能是中风的危险因素,也是中风后主要不良结局的早期指标。