Department of Radiology, Charité - Universitätsmedizin Berlin, Berlin, Germany.
Berlin Institute of Health at Charité - Universitätsmedizin Berlin, Berlin, Germany.
BMC Anesthesiol. 2024 Sep 5;24(1):308. doi: 10.1186/s12871-024-02687-3.
Critically ill patients with severe pancreatitis exhibit substantial muscle wasting, which limits in-hospital and post-hospital outcomes. Survivors of critical illness undergo extensive recovery processes. Previous studies have explored pancreatic function, quality of life, and costs post-hospitalization for AP patients, but none have comprehensively quantified muscle loss and recovery post-discharge. By applying an AI-based automated segmentation tool, we aimed to quantify muscle mass recovery in ICU patients after discharge.
Muscle segmentation was performed on 22 patients, with a minimum of three measurements taken during hospitalization and one clinically indicated examination after hospital discharge. Changes in psoas muscle area (PMA) between admission, discharge and follow up were calculated. T-Test was performed to identify significant differences between patients able and not able to recover their muscle mass.
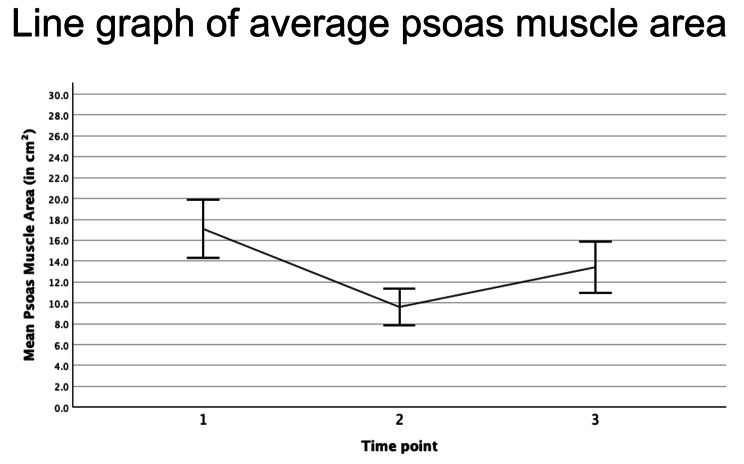
Monitoring PMA shows muscle loss during and gain after hospitalization: The mean PMA at the first scan before or at ICU admission (TP1) was 17.08 cm², at the last scan before discharge (TP2), mean PMA was 9.61 cm². The percentage change in PMA between TP1 and TP2 ranged from - 85.42% to -2.89%, with a mean change of -40.18%. The maximum muscle decay observed during the stay was - 50.61%. After a mean follow-up period of 438.73 days most patients (81%) were able to increase their muscle mass. Compared to muscle status at TP1, only 27% of patients exhibited full recovery, with the majority still presenting a deficit of 31.96%.
Muscle recovery in ICU patients suffering from severe AP is highly variable, with only about one third of patients recovering to their initial physical status. Opportunistic screening of post-ICU patient recovery using clinically indicated imaging and AI-based segmentation tools enables precise quantification of patients' muscle status and can be employed to identify individuals who fail to recover and would benefit from secondary rehabilitation. Understanding the dynamics of muscle atrophy may improve prognosis and support personalized patient care.
患有重症胰腺炎的危重症患者会出现明显的肌肉消耗,这会限制住院和出院后的结果。危重症幸存者会经历广泛的康复过程。之前的研究已经探讨了 AP 患者出院后的胰腺功能、生活质量和成本,但没有一项研究全面量化出院后的肌肉损失和恢复情况。通过应用基于人工智能的自动分割工具,我们旨在量化 ICU 患者出院后的肌肉量恢复情况。
对 22 名患者进行了肌肉分割,在住院期间至少进行了三次测量,在出院后进行了一次临床指示检查。计算入院时、出院时和随访时腰大肌面积(PMA)的变化。使用 T 检验来确定能够和不能恢复肌肉量的患者之间是否存在显著差异。
监测 PMA 显示出住院期间和出院后的肌肉损失和增加:第一次扫描(TP1)前或 ICU 入院时的平均 PMA 为 17.08 cm²,最后一次扫描(TP2)前出院时的平均 PMA 为 9.61 cm²。TP1 和 TP2 之间的 PMA 百分比变化范围从-85.42%到-2.89%,平均变化为-40.18%。在住院期间观察到的最大肌肉衰减为-50.61%。在平均随访 438.73 天后,大多数患者(81%)能够增加肌肉量。与 TP1 时的肌肉状态相比,只有 27%的患者完全恢复,大多数患者仍存在 31.96%的缺陷。
患有严重 AP 的 ICU 患者的肌肉恢复情况差异很大,只有约三分之一的患者能够恢复到最初的身体状态。使用临床指示成像和基于人工智能的分割工具对 ICU 后患者的恢复情况进行机会性筛查,可以精确量化患者的肌肉状况,并可以识别未能恢复的个体,从而为他们提供二次康复治疗。了解肌肉萎缩的动态变化可能会改善预后并支持个性化的患者护理。