Daniele Andrés J, Gregorietti Vanesa, Costa Diego, López-Fernández Teresa
Roffo Institute, Buenos Aires, Argentina.
Sanatorio Sagrado Corazón, Buenos Aires, Argentina.
Cardiooncology. 2024 Sep 5;10(1):58. doi: 10.1186/s40959-024-00260-y.
Anthracycline-based chemotherapy represents a cornerstone treatment for a number of common cancers, including breast cancer, lymphoma, and sarcoma. However, anthracycline-induced cardiotoxicity remains a significant concern, often presenting as a decline in cardiac function which can ultimately lead to heart failure (HF) or asymptomatic left ventricular dysfunction, in up to 10-15% of patients.Sodium-glucose transport protein 2 inhibitor (SGLT2i) therapies have been demonstrated to reduce the incidence of HF in high-risk non-cancer patients. Preliminary retrospective data suggest their role in mitigating the incidence of HF during or after anthracycline treatment METHODS: The EMPACARD-PILOT trial was a prospective case‒control study involving breast cancer patients scheduled to undergo anthracycline-based chemotherapy in a 4-cycle protocol of 60 mg/m2 doxorubicin. We used the HFA/ICOS risk score to identify patients at high or very high risk of cardiotoxicity. Patients with diabetes mellitus or stable heart failure with preserved ejection fraction (HFpEF) were prescribed empagliflozin (10 mg per day), starting seven days before the administration of anthracyclines and continuing for a period of six months. Those not meeting these criteria served as controls. The primary endpoint was cancer therapy-related cardiac dysfunction (CTRCD) incidence. CTRCD was defined as either a decrease in left ventricular ejection fraction (LVEF) of at least 10% to a final value below 50% or a reduction in global longitudinal strain (GLS) of at least 15% from baseline at any point during the study. The secondary endpoints included mortality and hospitalization due to cardiovascular causes or clinical heart failure. Exploratory endpoints included increases in serum troponin and NT-proBNP levels and a decrease in the glomerular filtration rate (GFR). The safety endpoints tracked includedketoacidosis, hypoglycemia, sepsis, neutropenic fever, and urinary tract infections.
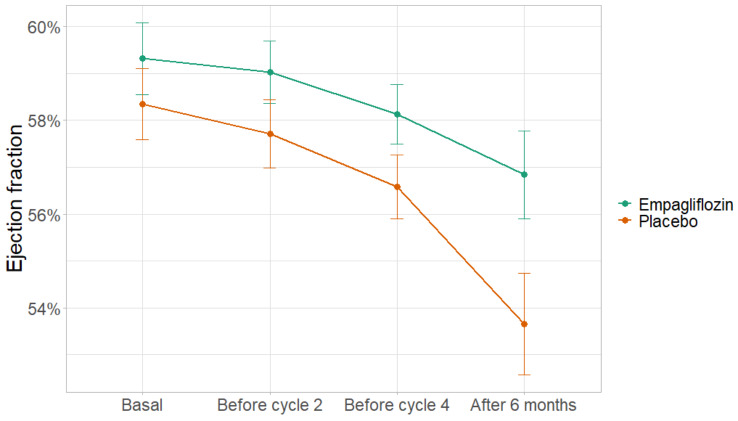
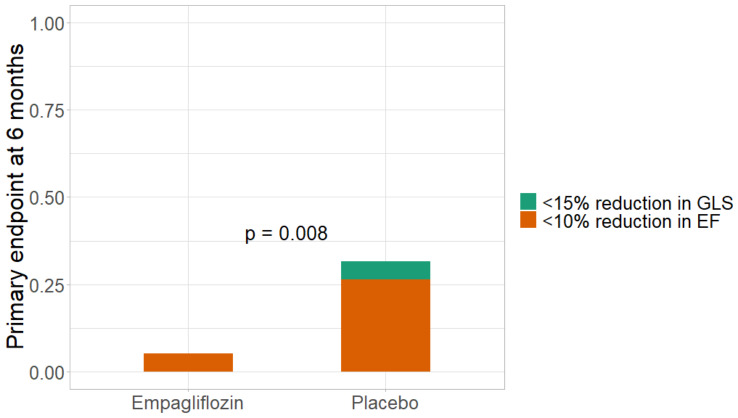
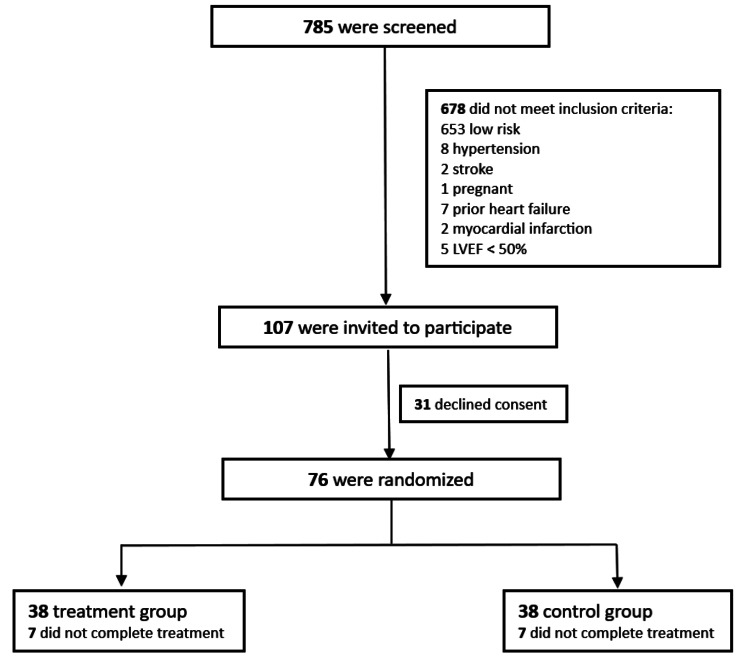
During the enrollment period, 785 breast cancer patients were analysed. Of these, 107 met the inclusion criteria, and 76 subsequently provided informed consent. The study was conducted with comparable adherence rates of 81.5% in both the empagliflozin group (n = 38) and the control group (n = 38). The follow-up data from 62 patients revealed a significant reduction in the primary outcome within 6 months for the empagliflozin group compared with the control group (6.5% vs. 35.5%, p = 0.005), with a relative risk of 0.18 (95% CI: 0.04-0.75). Compared with the control treatment, treatment with empagliflozin also significantly preserved the ejection fraction at 6 months follow-up (56.8% ± 5.8% vs. 53.7% ± 6.7, p = 0.029). However, there were no significant differences between the groups in terms of NT-proBNP, cTnI, clinical heart failure, GFR, or mortality/hospitalization due to heart failure.
Empagliflozin is associated with reduced incidence of CTRCD in high-risk patients treated with anthracyclines. These data should serve as the foundation for a clinical trial to test whether SGLT2 inhibitors can reduce the incidence of heart failure in this patient group.
基于蒽环类药物的化疗是多种常见癌症(包括乳腺癌、淋巴瘤和肉瘤)的基础治疗方法。然而,蒽环类药物引起的心脏毒性仍然是一个重大问题,通常表现为心脏功能下降,最终可导致高达10%-15%的患者出现心力衰竭(HF)或无症状左心室功能障碍。钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)疗法已被证明可降低高危非癌症患者HF的发生率。初步回顾性数据表明其在减轻蒽环类药物治疗期间或之后HF发生率方面的作用。方法:EMPACARD-PILOT试验是一项前瞻性病例对照研究,涉及计划接受以蒽环类药物为基础的化疗(60mg/m²阿霉素的4周期方案)的乳腺癌患者。我们使用HFA/ICOS风险评分来识别心脏毒性高风险或非常高风险的患者。患有糖尿病或射血分数保留的稳定心力衰竭(HFpEF)的患者在蒽环类药物给药前7天开始服用恩格列净(每日10mg),并持续6个月。不符合这些标准的患者作为对照。主要终点是癌症治疗相关的心脏功能障碍(CTRCD)发生率。CTRCD定义为左心室射血分数(LVEF)至少降低10%至最终值低于50%,或在研究期间任何时间点全球纵向应变(GLS)较基线至少降低15%。次要终点包括心血管原因或临床心力衰竭导致的死亡率和住院率。探索性终点包括血清肌钙蛋白和NT-proBNP水平升高以及肾小球滤过率(GFR)降低。跟踪的安全终点包括酮症酸中毒、低血糖、败血症、中性粒细胞减少性发热和尿路感染。
在入组期间,分析了785例乳腺癌患者。其中,107例符合纳入标准,76例随后提供了知情同意书。恩格列净组(n = 38)和对照组(n = 38)的研究依从率相当,均为81.5%。62例患者的随访数据显示,与对照组相比,恩格列净组在6个月内主要结局显著降低(6.5%对35.5%,p = 0.005),相对风险为0.18(95%CI:0.04 - 0.75)。与对照治疗相比,恩格列净治疗在6个月随访时也显著保留了射血分数(56.8%±5.8%对53.7%±6.7,p = 0.029)。然而,两组在NT-proBNP、cTnI、临床心力衰竭、GFR或心力衰竭导致的死亡率/住院率方面没有显著差异。
恩格列净与接受蒽环类药物治疗的高危患者CTRCD发生率降低相关。这些数据应作为临床试验的基础,以测试SGLT抑制剂是否可降低该患者群体的心力衰竭发生率。