Iqbal Muhammad Rafaih, Ari Kaso, Probert Spencer, Cai Wenyi, Ramadan Wafaa, Walton Sarah-Jane
Departments ofColorectal Surgery, Basildon University Hospital NHS Foundation Trust, Basildon.
General Surgery, Norfolk and Norwich University Hospital Hospital Foundation Trust.
Ann Med Surg (Lond). 2024 Aug 7;86(9):5024-5033. doi: 10.1097/MS9.0000000000002429. eCollection 2024 Sep.
Bowel cancer is a significant global health concern, ranking as the third most prevalent cancer worldwide. Laparoscopic resections have become a standard treatment modality for resectable colorectal cancer. This study aimed to compare the clinical and oncological outcomes of medial to lateral (ML) vs lateral to medial (LM) approaches in laparoscopic colorectal cancer resections.
A retrospective cohort study was conducted at a UK district general hospital from 2015 to 2019, including 402 patients meeting specific criteria. Demographic, clinical, operative, postoperative, and oncological data were collected. Participants were categorised into LM and ML groups. The primary outcome was 30-day complications, and secondary outcomes included operative duration, length of stay, lymph node harvest, and 3-year survival.
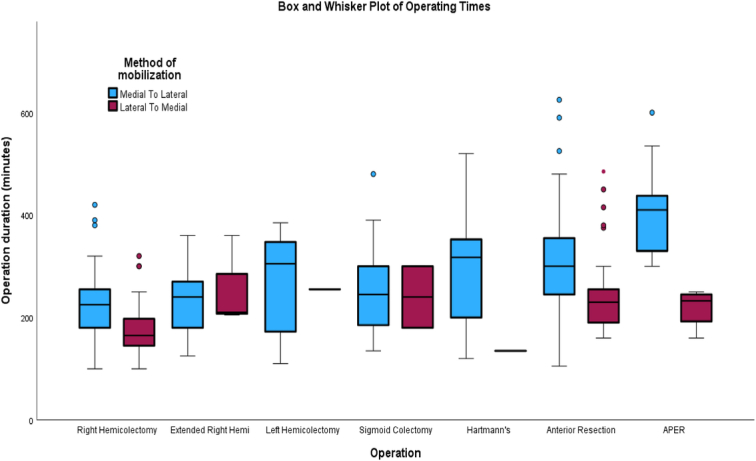
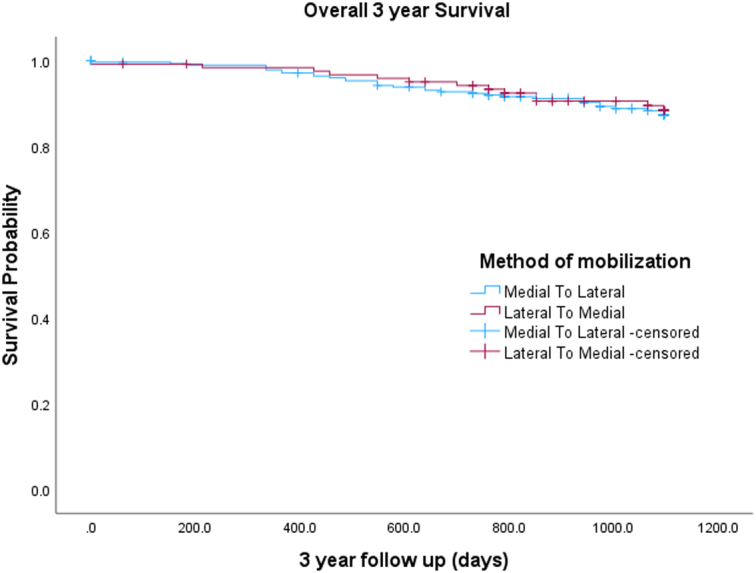
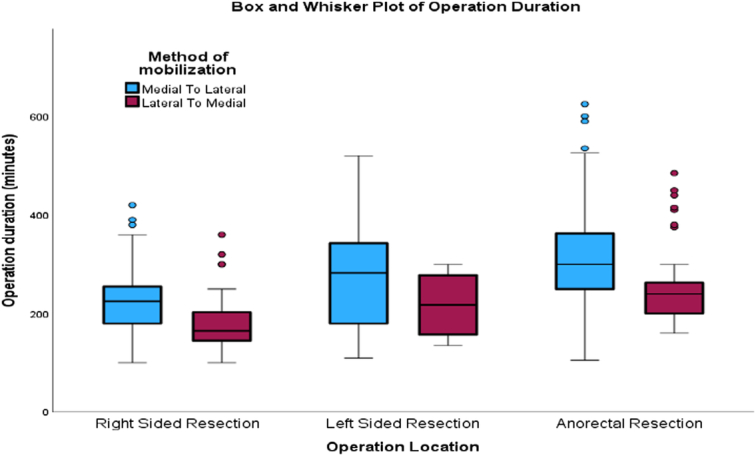
A total of 402 patients (55.7% males) were included: 102 (51.6% females) in the lateral mobilisation (LM) group and 280 (58.9% males) in the medial mobilisation (ML) group. Right hemicolectomy (=157, 39.1%) and anterior resection (=150, 37.3%) were the most performed procedures. The LM group had a shorter operative time for right hemicolectomy (median 165 vs. 225 min, <0.001) and anterior resection (median 230 vs. 300 min, <0.001). There was no significant difference between the two groups in terms of wound infection (=0.443), anastomotic leak (=0.981), postoperative ileus (=0.596), length of stay (=0.446), lymph node yield (=0.848) or 3-year overall survival rate (Log-rank 0.759).
The study contributes to the limited evidence on ML vs LM approaches. A shorter operative time in the LM group was noted in this study, contrary to some literature. Postoperative outcomes were comparable, with a non-significant increase in postoperative ileus in the LM group. The study emphasises the safety and feasibility of both approaches.
肠癌是一个重大的全球健康问题,在全球最常见的癌症中排名第三。腹腔镜切除术已成为可切除结直肠癌的标准治疗方式。本研究旨在比较腹腔镜结直肠癌切除术中从内侧到外侧(ML)与从外侧到内侧(LM)入路的临床和肿瘤学结果。
2015年至2019年在英国一家地区综合医院进行了一项回顾性队列研究,纳入402例符合特定标准的患者。收集了人口统计学、临床、手术、术后和肿瘤学数据。参与者被分为LM组和ML组。主要结局是30天并发症,次要结局包括手术时间、住院时间、淋巴结清扫数量和3年生存率。
共纳入402例患者(55.7%为男性):外侧游离(LM)组102例(51.6%为女性),内侧游离(ML)组280例(58.9%为男性)。右半结肠切除术(=157例,39.1%)和前切除术(=150例,37.3%)是最常进行的手术。LM组右半结肠切除术的手术时间较短(中位数165分钟对225分钟,<0.001),前切除术的手术时间也较短(中位数230分钟对300分钟,<0.001)。两组在伤口感染(=0.443)、吻合口漏(=0.981)、术后肠梗阻(=0.596)、住院时间(=0.446)、淋巴结获取数量(=0.848)或3年总生存率方面无显著差异(对数秩检验0.759)。
本研究为关于ML与LM入路的有限证据做出了贡献。本研究中注意到LM组手术时间较短,这与一些文献相反。术后结局具有可比性,LM组术后肠梗阻略有增加但不显著。该研究强调了两种入路的安全性和可行性。