Imashuku Yasuhiko, Hiraoka Susumu, Inoue Motoi, Mizuno Takayoshi, Oyagi Misuzu, Kitagawa Hirotoshi
Department of Anesthesiology, Shiga University of Medical Science, 5202192, Otsu, Shiga, Japan.
J Saudi Heart Assoc. 2024 Aug 17;36(3):232-236. doi: 10.37616/2212-5043.1390. eCollection 2024.
Atrial fibrillation after coronary artery bypass grafting is a relatively well known complication that has been observed for a long time. Though the management and drugs in the perioperative period have changed, their impact on the generation of postoperative atrial fibrillation remains unclear. Therefore, we investigated various perioperative management methods and the occurrence of postoperative atrial fibrillation.
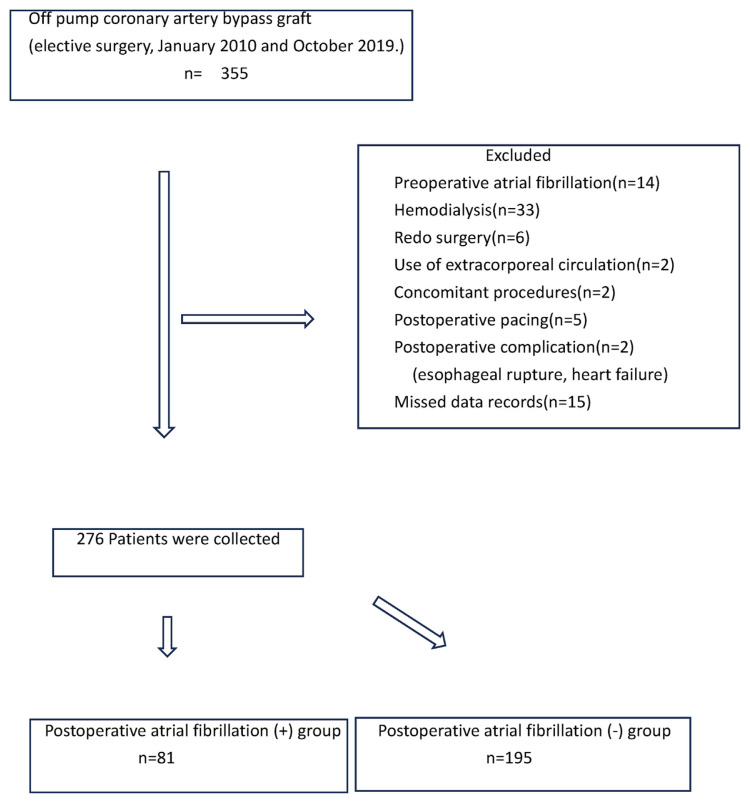
The patients underwent off-pump coronary artery bypass grafting between January 2010 and October 2019. The study was a retrospective observational study, and we investigated the incidence of atrial fibrillation during all 5 postoperative days. Patient factors included age, sex, height, and weight, preoperative factors included oral statin, HbA1c, left ventricular ejection fraction, and left atrial diameter; intraoperative factors included operation time, remifentanil use, beta-blocker use, magnesium-containing infusions use, in-out balance, and number of vascular anastomoses.
Postoperative atrial fibrillation was recognized in 81 out of 276 cases. There were significant differences between the two groups in terms of age, left atrial diameter, and intraoperative remifentanil use. A logistic regression analysis presented the effects of age (OR 1.045, 95% CI 1.015-1.076, P < 0.01), preoperative left atrial diameter (OR 1.072, 95% CI 1.023-1.124, P < 0.01), and intraoperative remifentanil use (OR 0.492, 95% CI 0.284-0.852, P = 0.011) on postoperative atrial fibrillation.
Operative time did not affect postoperative atrial fibrillation. Age and left atrial diameter had previously been shown to affect postoperative atrial fibrillation, and our results were similar. This study showed that the use of remifentanil reduced the incidence of postoperative atrial fibrillation. On the other hand, no other factors were found to have an effect.
冠状动脉搭桥术后房颤是一种早已为人所知且长期以来一直被观察到的并发症。尽管围手术期的管理和药物已经发生了变化,但其对术后房颤发生的影响仍不明确。因此,我们研究了各种围手术期管理方法与术后房颤的发生情况。
患者于2010年1月至2019年10月接受非体外循环冠状动脉搭桥术。该研究为回顾性观察性研究,我们调查了术后5天内房颤的发生率。患者因素包括年龄、性别、身高和体重,术前因素包括口服他汀类药物、糖化血红蛋白、左心室射血分数和左心房直径;术中因素包括手术时间、瑞芬太尼使用情况、β受体阻滞剂使用情况、含镁输注液使用情况、出入量平衡以及血管吻合数量。
276例患者中有81例被诊断为术后房颤。两组在年龄、左心房直径和术中瑞芬太尼使用情况方面存在显著差异。逻辑回归分析显示年龄(比值比1.045,95%置信区间1.015 - 1.076,P < 0.01)、术前左心房直径(比值比1.072,95%置信区间1.023 - 1.124,P < 0.01)和术中瑞芬太尼使用情况(比值比0.492,95%置信区间0.284 - 0.852,P = 0.011)对术后房颤的影响。
手术时间不影响术后房颤。年龄和左心房直径此前已被证明会影响术后房颤,我们的结果与之相似。本研究表明,瑞芬太尼的使用降低了术后房颤的发生率。另一方面,未发现其他因素有影响。