Department of Perioperative and Intensive Care, Intensive and Intermediate Care Unit, University of Helsinki and Helsinki University Hospital, P.O. Box 320, 00290 HUS, Helsinki, Finland.
Department of Anesthesia and Intensive Care, Hospital Nova of Central Finland, Central Finland Health Care District, Hoitajantie 3, 40620, Jyväskylä, Finland.
Sci Rep. 2024 Sep 6;14(1):20808. doi: 10.1038/s41598-024-71670-2.
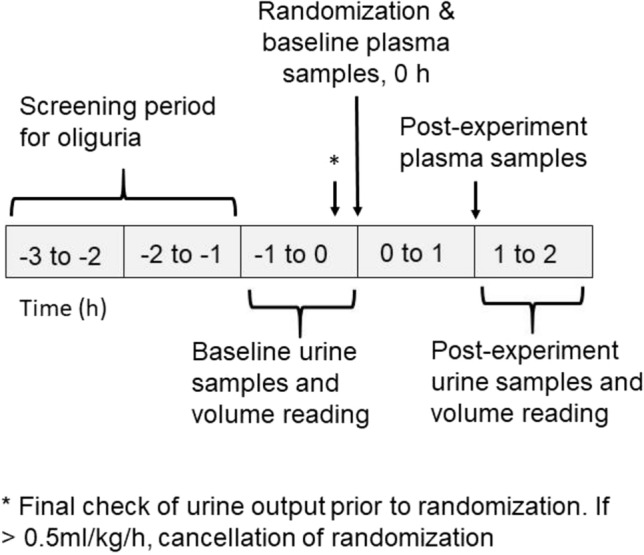
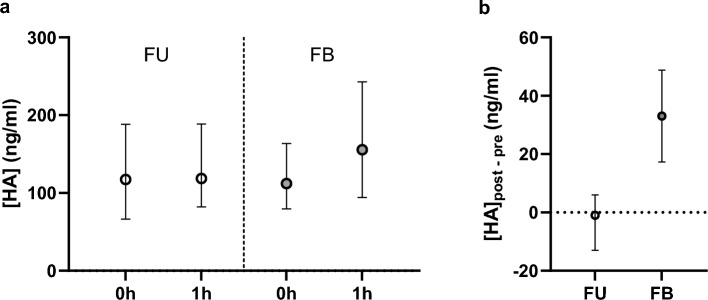
Fluid therapy is a fundamental part of supportive therapy in critical care. However, it is also a suspected risk for endothelial glycocalyx degradation which is associated with poor clinical outcomes. This secondary analysis of RESPONSE randomized trial compares the effect of follow-up strategy (FU) on endothelial biomarkers to that of 500 ml crystalloid fluid bolus (FB) in oliguric, hemodynamically optimized intensive care unit (ICU) patients. 130 adult subjects were enrolled in two Finnish ICUs from January 2017 to November 2020. Blood and urine samples of 63 patients in FU group and 67 patients in FB group were collected before and after the intervention and analyzed using enzyme-linked immunosorbent assays. Single fluid bolus, given after median of 3887 ml (interquartile range 2842; 5359 ml) resuscitation fluids in the preceding 24 h, increased plasma hyaluronan concentration compared to the follow-up strategy (difference in medians 29.2 ng/ml with 95% CI [14.5ng/ml; 55.5ng/ml], P < 0.001). No treatment effect was detected in the plasma levels of syndecan-1, , angiopoietin-2, angiopoietin receptors Tie2 and Tie1, or in soluble thrombomodulin in the adjusted median regression analysis. The increase in hyaluronan was independent of its simultaneous renal clearance but correlated moderately with the increase in endothelium-specific Tie1. The follow-up strategy did not show consistent endothelium-sparing effect but protected against hyaluronan increase. The mechanisms and consequences of hyaluronan fluctuations need further clarification. Trial registration: clinicaltrials.gov, NCT02860572. Registered 1 August 2016, https://www.clinicaltrials.gov/study/NCT02860572?term=NCT02860572&rank=1.
液体治疗是重症监护支持治疗的基础部分。然而,它也被怀疑会导致内皮糖萼降解,这与不良的临床结局有关。这项 RESPONSE 随机试验的二次分析比较了随访策略(FU)对内皮生物标志物的影响与 500ml 晶体液冲击量(FB)对少尿、血流动力学优化的重症监护病房(ICU)患者的影响。2017 年 1 月至 2020 年 11 月,芬兰的两家 ICU 共纳入了 130 名成年患者。FU 组的 63 例患者和 FB 组的 67 例患者在干预前后采集了血液和尿液样本,并用酶联免疫吸附试验进行了分析。与 FU 策略相比,在 24 小时前平均给予 3887ml(四分位间距 2842;5359ml)复苏液后,单次液体冲击使血浆透明质酸浓度增加(中位数差异为 29.2ng/ml,95%CI[14.5ng/ml;55.5ng/ml],P<0.001)。在调整后的中位数回归分析中,未检测到血浆中 syndecan-1、血管生成素-2、血管生成素受体 Tie2 和 Tie1 或可溶性血栓调节蛋白水平的治疗效果。透明质酸的增加与同时的肾清除无关,但与内皮特异性 Tie1 的增加中度相关。FU 策略没有表现出一致的内皮保护作用,但可以防止透明质酸的增加。透明质酸波动的机制和后果需要进一步阐明。试验注册:clinicaltrials.gov,NCT02860572。2016 年 8 月 1 日注册,https://www.clinicaltrials.gov/study/NCT02860572?term=NCT02860572&rank=1。