Siqueira-Neto Jair Lage, Lane Thomas R, Bernatchez Jean A, Calvet Alvarez Claudia Magalhaes, Barbosa da Silva Elany, Giardini Miriam A, Ekins Sean
Center for Discovery and Innovation in Parasitic Diseases, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of California, San Diego, La Jolla, California 92093, United States.
Collaborations Pharmaceuticals, Inc., 840 Main Campus Drive, Lab 3510, Raleigh, North Carolina 27606, United States.
ACS Omega. 2024 Aug 20;9(35):37288-37298. doi: 10.1021/acsomega.4c05060. eCollection 2024 Sep 3.
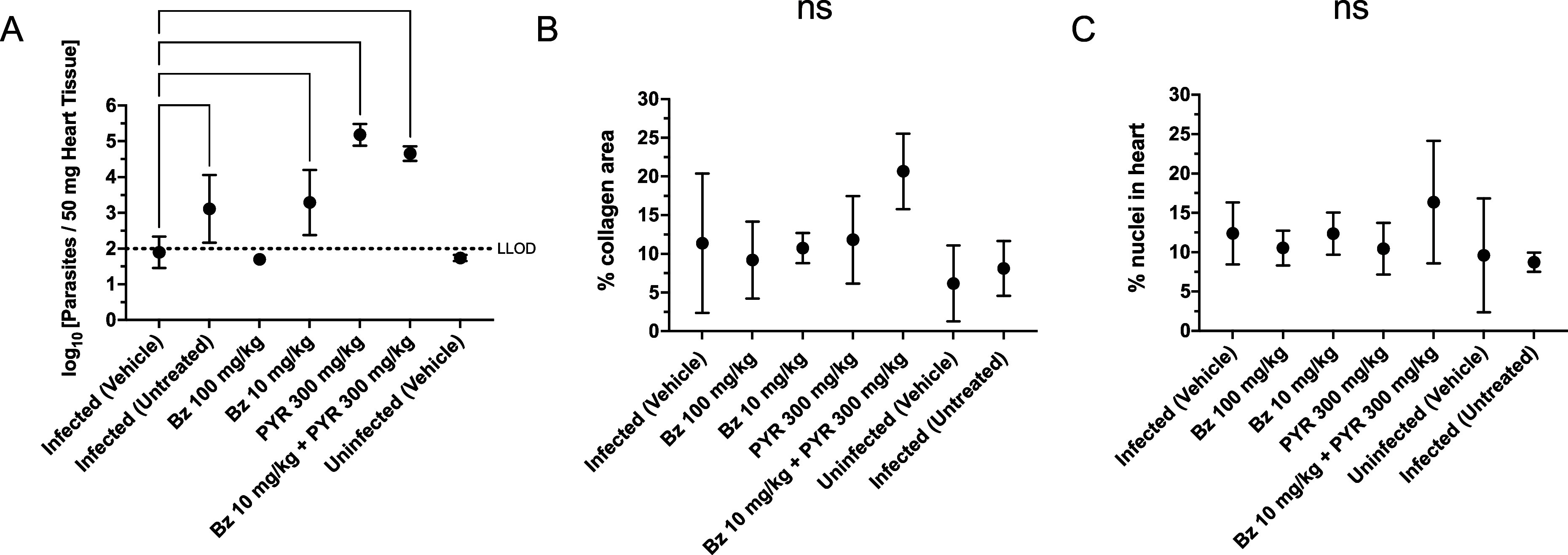
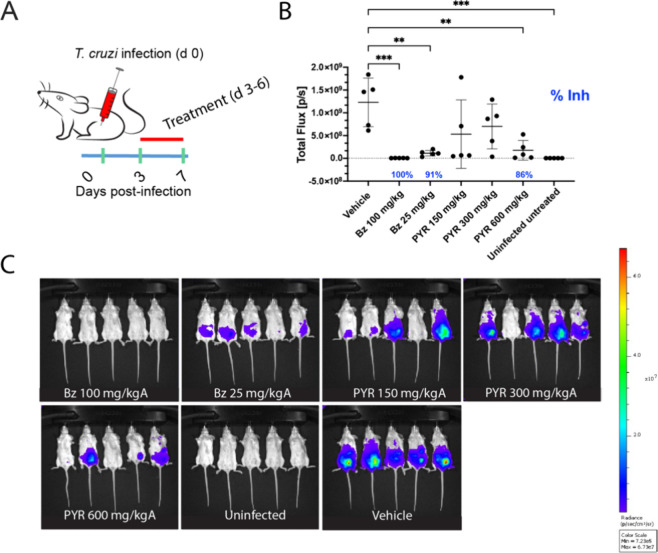
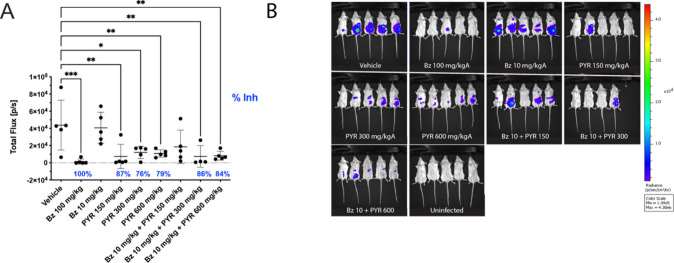
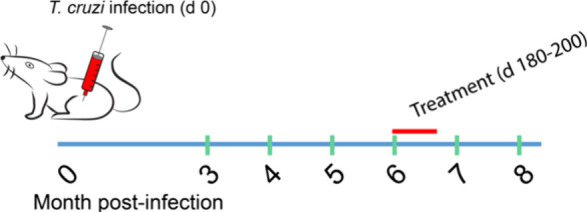
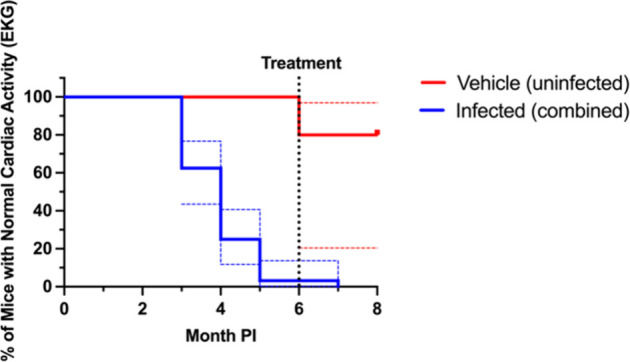
The eukaryotic parasite () is responsible for Chagas disease, which results in heart failure in patients. The disease is more common in Latin America, and is an emerging infection with The Centers for Disease Control estimating that greater than 300,000 people are currently infected in the United States. This disease has also spread from South and Central America, where it is endemic to many other countries, including Australia, Japan, and Spain. Current therapy for Chagas disease is inadequate due to limited efficacy in the indeterminate and chronic phases of the disease, in addition to the adverse effects from nifurtimox and benznidazole, which are nitro-containing drugs used for therapy. There is a clear need for new therapies for the Chagas disease. Using a computational machine learning approach, we have previously shown that the antimalarial pyronaridine tetraphosphate is active against Brazil-luc against parasites infecting a myoblast cell line and is also active in an acute mouse model of Chagas disease when dosed i.p. We now further evaluated oral pyronaridine as a monotherapy to determine the minimum effective dose to treat acute and chronic models of Chagas disease. Our results for Brazil-luc demonstrated daily oral dosing with pyronaridine from 150 to 600 mg/kg resulted in statistically significant inhibition in the 7 day acute mouse model. Combination therapy with daily dosing of benznidazole and pyronaridine in the acute infection model demonstrated that 300 mg/kg pyronaridine could return statistically significant antiparasitic activity to a subtherapetic 10 mg/kg benznidazole. In contrast, pyronaridine as monotherapy or combined with benznidazole lacked efficacy in the chronic mouse model, whereas 100 mg/kg benznidazole alone demonstrated undetectable parasites in the heart of mice. Pyronaridine requires further assessment in other chronic models to identify if it can be used beyond the acute stage of infection.
真核寄生虫()是恰加斯病的病原体,该病会导致患者心力衰竭。这种疾病在拉丁美洲更为常见,并且是一种新出现的感染病,美国疾病控制中心估计目前美国有超过30万人感染。这种疾病也已从南美洲和中美洲传播到包括澳大利亚、日本和西班牙在内的许多其他国家,在这些国家呈地方性流行。由于在疾病的不确定期和慢性期疗效有限,以及用于治疗的硝呋替莫和苯硝唑(含硝基的药物)会产生不良反应,目前针对恰加斯病的治疗方法并不充分。显然需要针对恰加斯病的新疗法。我们之前使用计算机机器学习方法表明,抗疟药物磷酸咯萘啶对巴西 - 荧光素酶(Brazil - luc)在感染成肌细胞系的寄生虫中具有活性,并且在恰加斯病急性小鼠模型中腹腔注射给药时也具有活性。我们现在进一步评估口服磷酸咯萘啶作为单一疗法,以确定治疗恰加斯病急性和慢性模型的最小有效剂量。我们针对巴西 - 荧光素酶的研究结果表明,在7天急性小鼠模型中,每天口服150至600毫克/千克的磷酸咯萘啶可产生具有统计学意义的抑制作用。在急性感染模型中,每天联合使用苯硝唑和磷酸咯萘啶进行治疗表明,300毫克/千克的磷酸咯萘啶可使低于治疗剂量的10毫克/千克苯硝唑恢复具有统计学意义的抗寄生虫活性。相比之下,磷酸咯萘啶作为单一疗法或与苯硝唑联合使用在慢性小鼠模型中缺乏疗效,而单独使用100毫克/千克苯硝唑在小鼠心脏中未检测到寄生虫。磷酸咯萘啶需要在其他慢性模型中进一步评估,以确定它是否可以在感染的急性期之后使用。