Nguyen Dung Viet, Le Thanh Ngoc, Truong Binh Quang, Nguyen Hoai Thi Thu
Department of Internal Medicine, VNU University of Medicine and Pharmacy, Hanoi, Vietnam.
VNU University of Medicine and Pharmacy, Hanoi, Vietnam.
Eur J Heart Fail. 2025 Jan;27(1):72-84. doi: 10.1002/ejhf.3454. Epub 2024 Sep 9.
Angiotensin receptor-neprilysin inhibitor (ARNI) has played an increasingly important role in the management of heart failure (HF). However, the evidence on the benefits of ARNI in HF patients with end-stage kidney disease (ESKD) undergoing dialysis is limited. This study aimed to investigate the efficacy and safety of ARNI in patients with concomitant HF and ESKD on maintenance dialysis.
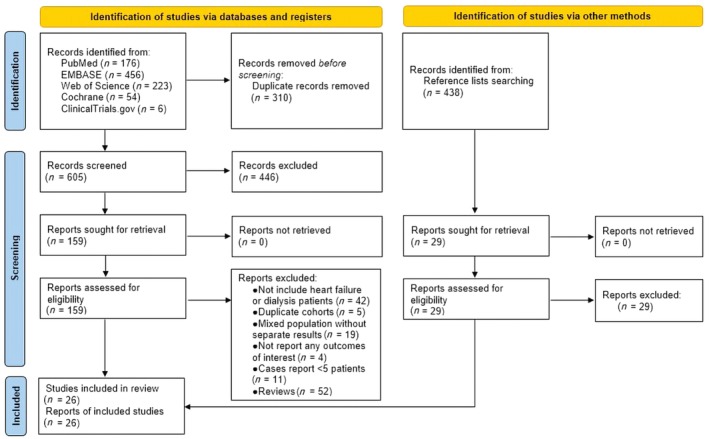
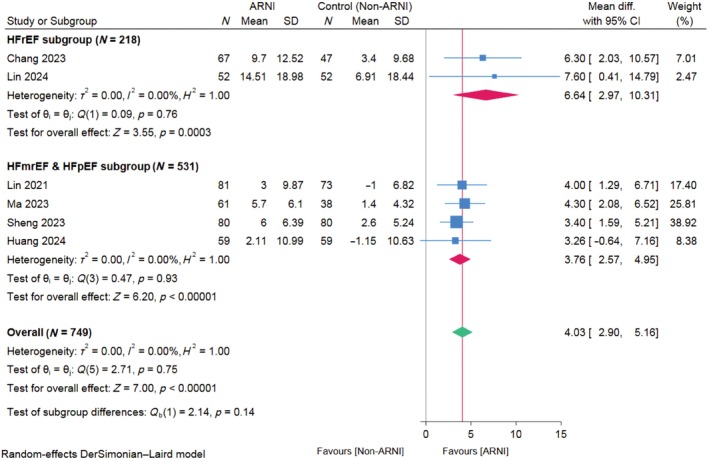
We systematically searched the MEDLINE, Embase, Web of Science, Cochrane, and ClinicalTrials.gov databases for studies reporting outcomes after ARNI treatment in HF patients with ESKD on dialysis. All meta-analyses were performed using the random effects model. Twenty-six studies comprising 2494 patients with concomitant HF and ESKD undergoing dialysis were included. Our synthesis showed a significant improvement in left ventricular ejection fraction (LVEF) between before and after ARNI treatment (mean change: 8.05%; 95% confidence interval [CI] 5.57-10.54). Compared to the conventional group, the ARNI group showed a greater improvement in LVEF (mean difference: 4.03%; 95% CI 2.90-5.16). This effect was more pronounced in patients with HF with reduced ejection fraction (p < 0.0001). Patients treated with ARNI had a lower risk of all-cause mortality (risk ratio [RR] 0.64; 95% CI 0.45-0.92; p = 0.01) but had a similar rate of HF hospitalization (RR 0.71; 95% CI 0.43-1.18; p = 0.19). ARNI treatment showed benefits in the improvement of left ventricular end-systolic diameter, left ventricular mass index, left atrial diameter, and E/e' ratio (p < 0.05), while it did not significantly increase the risk of severe hyperkalaemia (p = 0.33) or symptomatic hypotension (p = 0.53).
This meta-analysis provided insights into the benefits of ARNI in HF patients with ESKD undergoing dialysis by improving left ventricular function, reversing left ventricular remodelling, and reducing the risk of all-cause mortality, without increasing the risk of HF hospitalizations, severe hyperkalaemia, and symptomatic hypotension.
血管紧张素受体脑啡肽酶抑制剂(ARNI)在心力衰竭(HF)的管理中发挥着越来越重要的作用。然而,关于ARNI对接受透析的终末期肾病(ESKD)心力衰竭患者益处的证据有限。本研究旨在探讨ARNI对维持性透析的合并HF和ESKD患者的疗效和安全性。
我们系统检索了MEDLINE、Embase、Web of Science、Cochrane和ClinicalTrials.gov数据库,以查找关于ARNI治疗透析的ESKD心力衰竭患者后结局的研究。所有荟萃分析均采用随机效应模型。纳入了26项研究,共2494例合并HF和ESKD且正在接受透析的患者。我们的综合分析显示,ARNI治疗前后左心室射血分数(LVEF)有显著改善(平均变化:8.05%;95%置信区间[CI] 5.57 - 10.54)。与传统治疗组相比,ARNI组的LVEF改善更大(平均差异:4.03%;95% CI 2.90 - 5.16)。这种效应在射血分数降低的HF患者中更为明显(p < 0.0001)。接受ARNI治疗的患者全因死亡风险较低(风险比[RR] 0.64;95% CI 0.45 - 0.92;p = 0.01),但心力衰竭住院率相似(RR 0.71;95% CI 0.43 - 1.18;p = 0.19)。ARNI治疗在改善左心室收缩末期内径、左心室质量指数、左心房内径和E/e'比值方面显示出益处(p < 0.05),同时并未显著增加严重高钾血症风险(p = 0.33)或症状性低血压风险(p = 0.53)。
这项荟萃分析通过改善左心室功能、逆转左心室重构以及降低全因死亡风险,同时不增加心力衰竭住院、严重高钾血症和症状性低血压风险,揭示了ARNI对接受透析的ESKD心力衰竭患者的益处。