Byakwaga Helen, Semeere Aggrey, Laker-Oketta Miriam, Busakhala Naftali, Freeman Esther, Rotich Elyne, Wenger Megan, Kadama-Makanga Philippa, Kisuya Job, Semakadde Matthew, Mwine Bronia, Kasozi Charles, Mwebesa Bwana, Maurer Toby, Glidden David V, Wools-Kaloustian Kara, Kambugu Andrew, Martin Jeffrey
Infectious Disease Institute, Makerere University College of Health Sciences, Kampala, Uganda.
Academic Model Providing Access to Healthcare (AMPATH), Eldoret, Kenya.
medRxiv. 2024 Aug 28:2024.08.26.24312536. doi: 10.1101/2024.08.26.24312536.
Despite widespread access to antiretroviral therapy (ART) in the "Treat All" era, HIV-associated Kaposi sarcoma (KS) remains among the most common malignancies in sub-Saharan Africa. Survival after KS diagnosis has historically been poor in Africa, but knowledge whether survival has changed at the population level in the contemporary era has been limited by lack of community-representative surveillance and monitoring systems.
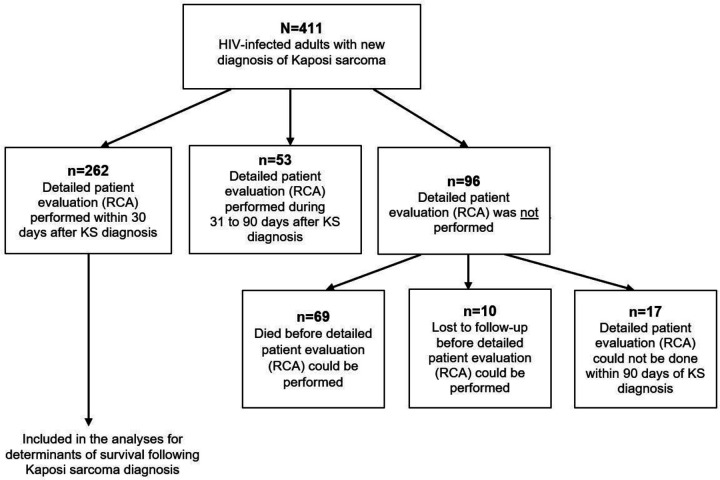
We identified all adult persons living with HIV (PLWH) with a new diagnosis of KS made between 2016 and 2019 during outpatient or inpatient care at prototypical primary care-providing medical facilities in Kenya and Uganda using rapid case ascertainment. Participants were subsequently followed for vital status, including community tracking for those who became lost to follow-up.
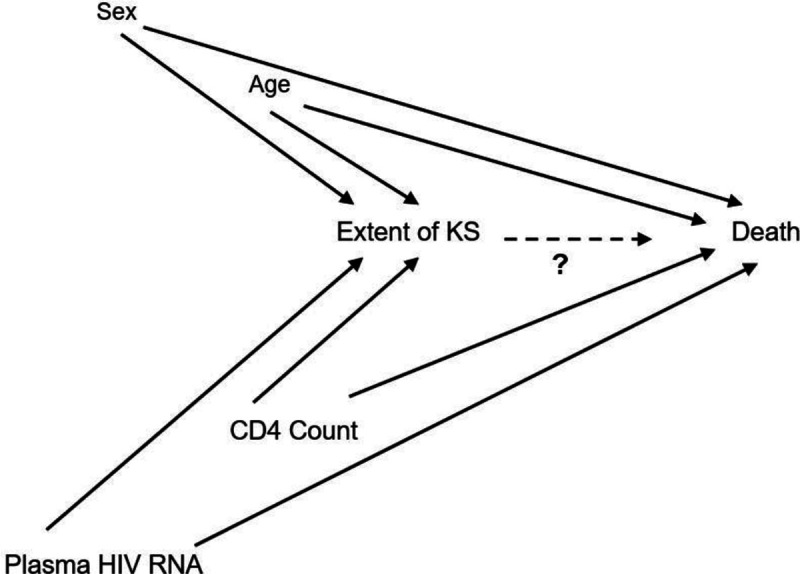
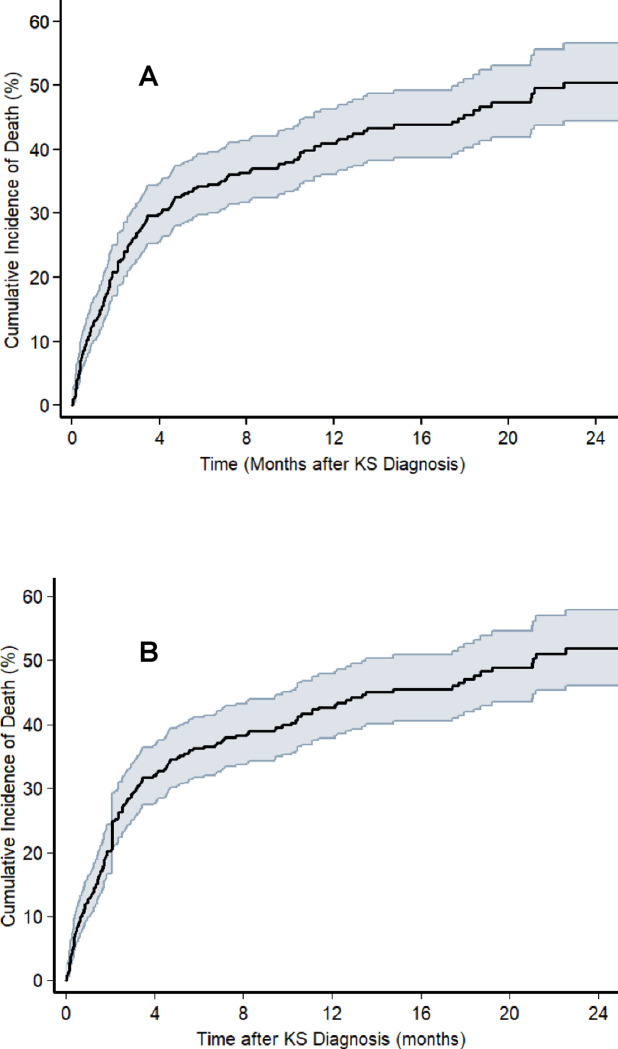
Among 411 participants with newly diagnosed KS, 71% were men, median age was 34 (IQR: 30 to 41) years, and 91% had ACTG T1 tumor extent. Over a median follow-up of 7.8 (IQR: 2.4 to 17.9) months, cumulative incidence of death (95% CI) at months 6, 12 and 18 were 34% (30% to 39%), 41% (36% to 46%) and 45% (40% to 51%), respectively. Having the highest number of anatomic sites (11 to 16) harboring KS lesions (hazard ratio 2.2 (95% CI: 1.3-3.8) compared to 1 to 3 sites) and presence of oral KS lesions (hazard ratio 2.2 (95% CI: 1.4-3.3)) were independently associated with higher mortality. Lower hemoglobin and CD4 count as well as higher plasma HIV RNA were also associated with higher mortality.
Among PLWH with newly diagnosed KS in East Africa in the "Treat All" era, survival was poor and related to mucocutaneous extent of KS. The findings emphasize the need for better control of KS in Africa, including novel approaches for earlier detection, better linkage to oncologic care, and more potent therapy.
在“全面治疗”时代,尽管抗逆转录病毒疗法(ART)已广泛普及,但在撒哈拉以南非洲地区,与人类免疫缺陷病毒(HIV)相关的卡波西肉瘤(KS)仍是最常见的恶性肿瘤之一。历史上,非洲地区KS诊断后的生存率一直很低,但由于缺乏具有社区代表性的监测系统,目前尚不清楚当代人群水平的生存率是否发生了变化。
我们通过快速病例确诊,确定了2016年至2019年间在肯尼亚和乌干达提供初级医疗服务的典型医疗机构门诊或住院治疗期间新诊断为KS的所有成年HIV感染者(PLWH)。随后对参与者进行生命状态随访,包括对失访者进行社区追踪。
在411例新诊断为KS的参与者中,71%为男性,中位年龄为34岁(四分位间距:30至41岁),91%的患者ACTG T1肿瘤分期。在中位随访7.8个月(四分位间距:2.4至17.9个月)期间,第6、12和18个月的累积死亡发生率(95%置信区间)分别为34%(30%至39%)、41%(36%至46%)和45%(40%至51%)。KS病变累及的解剖部位数量最多(11至16个)(与1至3个部位相比,风险比为2.2(95%置信区间:1.3 - 3.8))以及存在口腔KS病变(风险比为2.2(95%置信区间:1.4 - 3.3))与较高的死亡率独立相关。较低的血红蛋白和CD4细胞计数以及较高的血浆HIV RNA水平也与较高的死亡率相关。
在“全面治疗”时代东非新诊断为KS的PLWH中,生存率较低,且与KS的皮肤黏膜累及范围有关。研究结果强调了在非洲更好地控制KS的必要性,包括采用新方法进行早期检测、更好地与肿瘤治疗相衔接以及更有效的治疗。