Department of General Pediatrics and Neonatology, Universities of Giessen and Marburg Lung Center, Member of the German Center for Lung Research, Justus-Liebig-University Giessen, Giessen, Germany.
Federal State Consortium of Quality Assurance Hesse, Eschborn, Germany.
JAMA Netw Open. 2024 Sep 3;7(9):e2432438. doi: 10.1001/jamanetworkopen.2024.32438.
Population-based analyses provided divergent data on the changes in preterm birth rates during the COVID-19 pandemic, and there is a gap of knowledge on the variations in birth characteristics.
To study changes in perinatal care, causes of preterm delivery, and very preterm (VPT; defined as <32 weeks' gestation) birth rates before and during the COVID-19 pandemic.
DESIGN, SETTING, AND PARTICIPANTS: This population-level cohort study used data from the quality assurance registry, which covers all births in Hesse, Germany. Deliveries during the COVID-19 pandemic (2020) were compared with the corresponding grouped prepandemic time intervals (2017 to 2019). Analyses were executed between August 2023 and July 2024.
Analyses were directed to study differences in preterm births before and during 3 pandemic phases: first (March 14 to May 15, 2020) and second (October 19 to December 31, 2020) lockdowns and a period of less-vigorous restrictions between them (May 16 to October 18, 2020).
Outcomes of interest were variations in preterm birth rates in the context of baseline characteristics and causes of preterm births during vs before the first year of the COVID-19 pandemic.
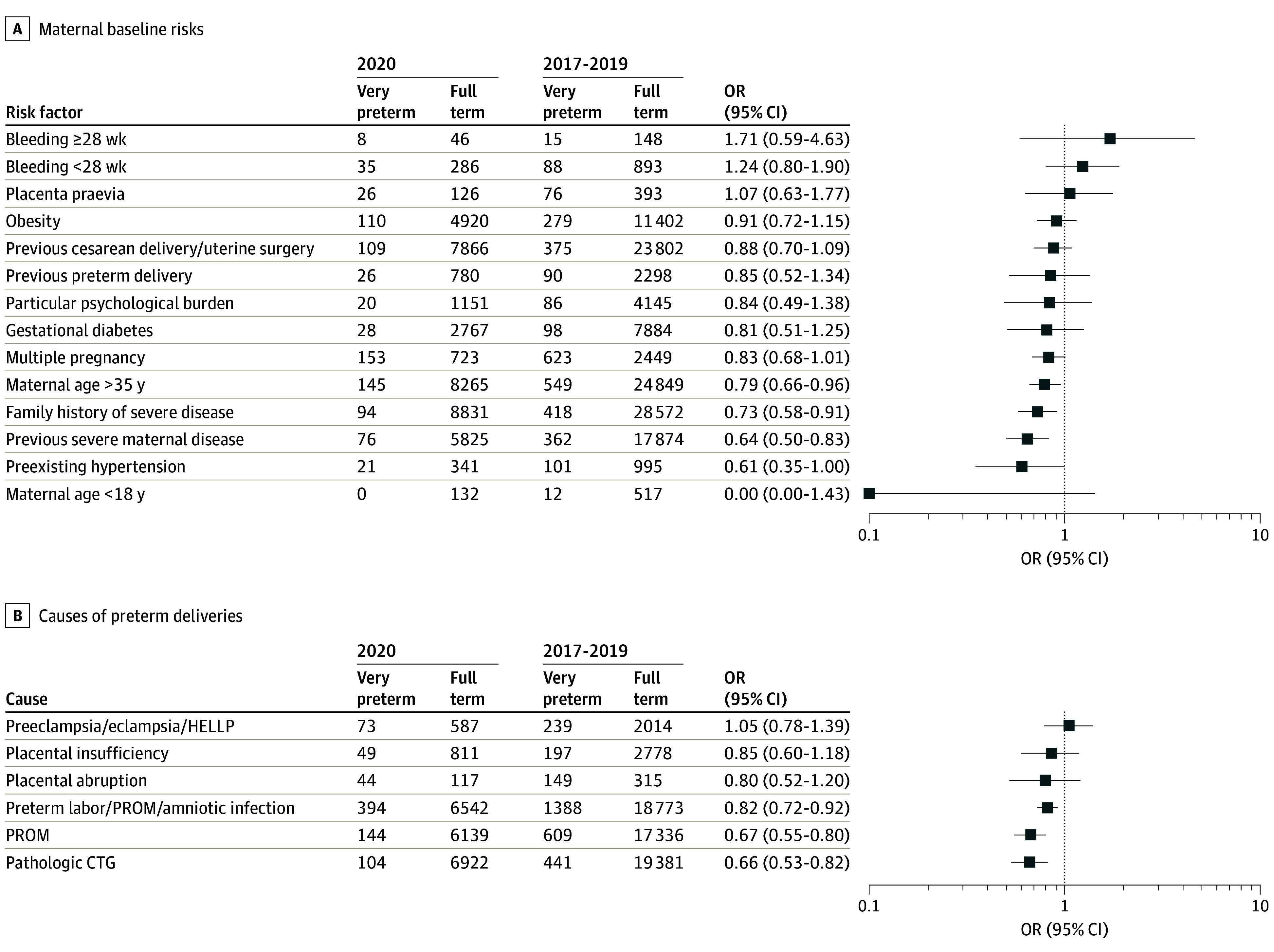
From the total cohort of 184 827 births from 2017 to 2020, 719 stillbirths occurred and 184 108 infants were liveborn. Compared with the prepandemic period, medical care characteristics did not differ during the COVID-19 period. The odds of VPT births were lower during the pandemic period (odds ratio [OR], 0.87; 95% CI, 0.79-0.95) compared with the prepandemic period, with the greatest reduction observed during the second lockdown period (OR, 0.69; 95% CI, 0.55-0.84). Reduction in VPT births was attributed to fewer births in pregnancies among individuals with a history of serious disease (OR, 0.64; 95% CI, 0.50-0.83), pathologic cardiotocography (OR, 0.66; 95% CI, 0.53-0.82), and intrauterine infection (OR, 0.82; 95% CI, 0.72-0.92) while incidences of history of preterm birth, multiple pregnancies, serious or severe psychological distress, and preeclampsia, eclampsia, or hemolysis, elevated liver enzymes, and low platelet count syndrome as cause for preterm delivery remained unchanged.
In this population-based cohort study on the COVID-19 pandemic and preterm birth rates, the duration of exposure to mitigation measures during pregnancy was associated with accelerated reductions in preterm births. The findings of lower rates of baseline risks and causes of preterm deliveries support efforts to intensify health care prevention programs during pregnancy to reduce the preterm birth burden. These findings of this study put particular focus on hygiene measures to reduce the rate of deliveries for intrauterine infection and highlight the potential of expanding strategies to the different risks and causes of preterm delivery.
基于人群的分析提供了关于 COVID-19 大流行期间早产率变化的不同数据,并且在出生特征的变化方面存在知识差距。
研究 COVID-19 大流行前后围产期护理、早产原因和极早产(定义为<32 周妊娠)发生率的变化。
设计、地点和参与者:这项基于人群的队列研究使用了质量保证登记处的数据,该登记处涵盖了德国黑森州的所有分娩。将大流行期间(2020 年)的分娩与相应的分组流行前时间间隔(2017 年至 2019 年)进行比较。分析于 2023 年 8 月至 2024 年 7 月之间进行。
分析针对早产率在以下三个大流行阶段的差异进行了定向研究:第一阶段(2020 年 3 月 14 日至 5 月 15 日)和第二阶段(2020 年 10 月 19 日至 12 月 31 日)封锁以及其间限制程度较低的阶段(2020 年 5 月 16 日至 10 月 18 日)。
感兴趣的结果是在大流行前一年的背景下,根据基线特征和早产原因,早产率的变化。
在 2017 年至 2020 年的总共 184827 次分娩中,发生了 719 例死产,184108 例婴儿存活。与流行前时期相比,COVID-19 期间的医疗保健特征没有差异。与流行前时期相比,极早产的分娩几率在大流行期间较低(比值比 [OR],0.87;95%置信区间,0.79-0.95),在第二阶段封锁期间降幅最大(OR,0.69;95%置信区间,0.55-0.84)。极早产分娩率的降低归因于有严重疾病史的妊娠中分娩减少(OR,0.64;95%置信区间,0.50-0.83)、病理性胎心监护(OR,0.66;95%置信区间,0.53-0.82)和宫内感染(OR,0.82;95%置信区间,0.72-0.92),而早产史、多胎妊娠、严重或严重心理困扰以及子痫前期、子痫或溶血、肝酶升高和血小板计数降低综合征作为早产原因的发生率保持不变。
在这项关于 COVID-19 大流行和早产率的基于人群的队列研究中,怀孕期间接触缓解措施的持续时间与早产率的加速下降有关。较低的基线风险和早产原因发生率的发现支持在怀孕期间加强卫生保健预防计划以减少早产负担的努力。本研究的这些发现特别关注减少宫内感染分娩率的卫生措施,并强调扩大策略以应对不同的早产风险和原因的潜力。